The average care seeker interacts with 7 to 13 pieces of content before converting into a qualified lead. That figure, drawn from cross-industry B2B conversion research, means your home care agency’s last-click Google Ads report captures roughly 1 of those 13 touchpoints and calls it the whole story.
TL;DR: Home care leads touch 7-13 content pieces across multiple channels before converting. Agencies that rely on last-touch attribution (giving 100% credit to the final click) systematically undervalue top-of-funnel channels like content marketing and SEO, often cutting budgets that feed the very pipeline they depend on. Multi-touch attribution models distribute credit more accurately, but each model carries its own distortions.
Last-Touch Attribution Gives You a Distorted Budget
When your reporting dashboard credits 100% of a conversion to the final interaction, typically a branded Google search or a retargeting ad click, every dollar you’ve spent building awareness disappears from the ROI calculation. Research on healthcare attribution modeling from Best BMA’s January 2026 analysis puts it plainly: “Models shape budgeting decisions, dramatically.” The model you choose determines which channels look profitable and which look like waste.
The downstream consequence is predictable. An agency sees that Google Ads for care providers generated 40 leads this quarter with a cost-per-lead of $85 and concludes paid search is the winner. The blog, which drove 0 direct conversions by last-touch count, gets its content budget slashed by 50%. But 70% of those bottom-funnel converters had their first interaction through content, according to cross-industry attribution benchmarks. Cut that spend, and your pipeline can collapse within 3 to 6 months as the top of the funnel dries up.
The Senior Care Customer Journey Has Two Decision-Makers
Why is multi-channel conversion tracking especially unreliable in home care? Because the person researching services at 11pm on their phone is usually not the person receiving care. Adult children search Google, read blog posts, compare reviews on A Place for Mom, and forward links to siblings via group text. The senior, meanwhile, responds to a direct mail piece or a referral from their physician.
Customer Centric Solutions LLC identifies five distinct lenses for evaluating the senior living and care journey: customer motivation, customer expectations, moments of truth, customer emotions, and customer effort. Each lens shifts depending on whether you’re tracking the adult child or the senior. Multi-stakeholder marketing for home care requires building at least 2 separate follow-up sequences: one optimized for phone calls and simple text messages (the senior), and another optimized for email and scheduling links (the adult child).
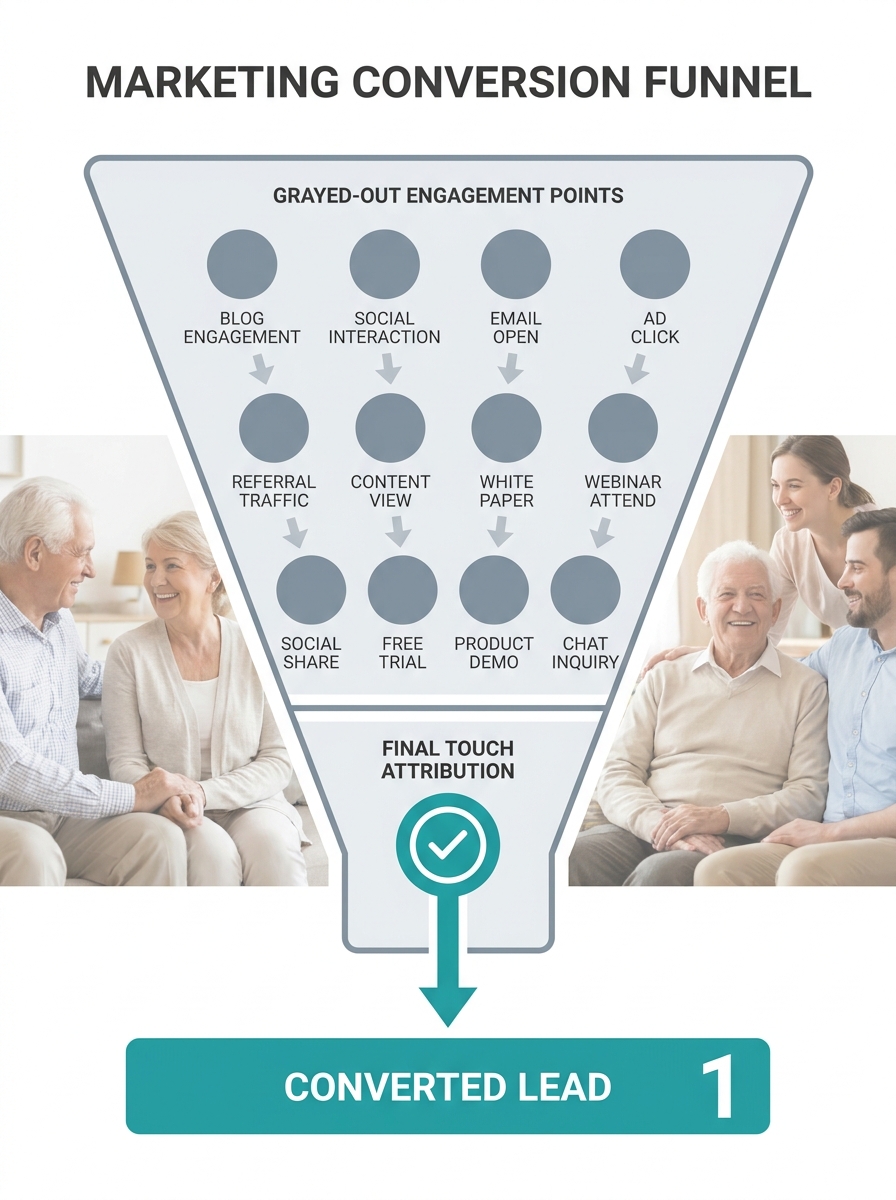
This two-audience problem breaks standard attribution in a specific way. The adult daughter clicks a Facebook ad (touchpoint 1), reads 3 blog posts over 2 weeks (touchpoints 2 through 4), opens an email nurture sequence twice (touchpoints 5 and 6), then hands the phone to her mother, who calls your intake line directly. Your CRM logs a phone lead with no digital trail. Six marketing touchpoints vanish. If your agency has invested in email marketing for care providers, those nurture touches contributed real value, but your reporting system can’t prove it without identity resolution connecting the daughter’s browsing session to the mother’s phone call.

Five Attribution Models and What Each One Distorts
Every attribution model answers the question “which channel deserves credit?” differently. And every answer carries a built-in bias. Seven Figure Agency’s breakdown of 15 attribution models warns that position-based approaches “may oversimplify complex consumer behavior patterns, potentially missing important nuances in the customer journey.”
Here’s how the five most common models distribute credit across a 7-touchpoint home care conversion path:
| Model | Credit to First Touch | Credit to Middle Touches | Credit to Last Touch | Best Use Case | Biggest Blind Spot |
|---|---|---|---|---|---|
| Last-Touch | 0% | 0% | 100% | Measuring direct-response campaigns | Ignores all awareness and nurture activity |
| First-Touch | 100% | 0% | 0% | Identifying top-of-funnel winners | Ignores conversion-driving channels |
| Linear | 14.3% each | 14.3% each | 14.3% | Understanding full funnel involvement | Treats a casual blog visit the same as a consultation booking |
| U-Shaped (Position-Based) | 40% | 20% split across middle | 40% | Balancing acquisition and conversion | Undervalues mid-funnel nurture sequences |
| W-Shaped | 30% | 30% to key middle touch, 10% distributed | 30% | Complex journeys with a clear mid-point event | Requires manual definition of the “key” middle event |
The W-shaped model, described in SocialClimb’s healthcare attribution guide, assigns 30% credit to the initial touchpoint (say, a blog post found through organic search), 30% to a key mid-funnel event (a webinar or guide download), and 30% to the final conversion trigger, with the remaining 10% distributed across everything else. For a home care agency running home care SEO, paid search, email nurture, and referral partnerships simultaneously, this model captures 90% of the credit in 3 defined moments. Everything in between, the retargeting impressions, the Google Business Profile views, the second and third email opens, splits that thin 10%.
Every attribution model answers the question “which channel deserves credit?” differently. And every answer carries a built-in bias.
Connecting CRM Data to Close the Identity Gap
The technology problem underlying home care marketing attribution is identity resolution. Cookie-based tracking fragments the customer journey across devices and sessions. An adult child who searches “home care near me” on her phone at lunch, reads your blog on her work laptop, and then calls from her personal phone looks like 3 separate anonymous visitors in Google Analytics.
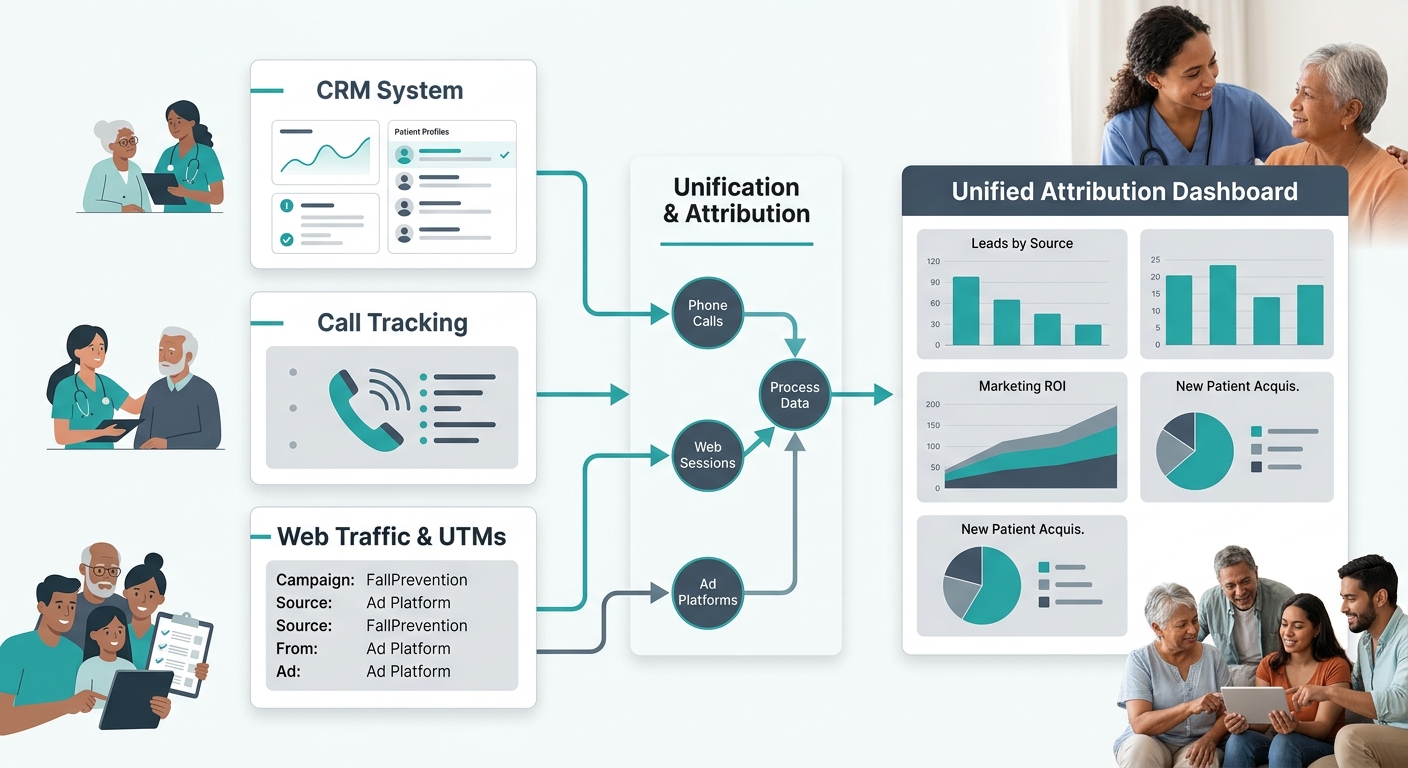
Patient Prism’s 2026 comparison of healthcare attribution tools highlights that effective platforms “unify data from marketing tools, CRM systems, and advertising platforms to provide attribution modeling and revenue forecasting.” But the report also flags a specific gap: most general-purpose attribution platforms lack healthcare-specific features like patient interaction tracking and clinical intent identification.
For home care agencies, the practical fix involves 3 integrations:
- CRM-to-ad-platform sync so that when a lead converts to a paying client (often 2 to 8 weeks after first inquiry), that revenue data flows back to Google Ads and Facebook, correcting the cost-per-acquisition numbers retroactively.
- Call tracking with speech analytics that tags whether a call was about placing someone into care, what service line was discussed, and whether the caller was the senior or a family member. Agencies using call recording data to identify drop-off points gain a clearer picture of which calls originated from which campaigns.
- UTM parameter discipline across every link in every channel, including the links inside referral partner emails, the URLs on printed materials (use unique landing pages or QR codes), and the links in your Google Business Profile posts.
Without all 3, your attribution data has structural holes. With them, you can trace at least 60 to 80% of touchpoints back to a channel, a significant improvement over the 15 to 25% visibility that last-touch reporting provides alone.
Where the Models Break Down for Referral-Driven Agencies
Home care agencies with strong referral networks face an attribution problem that no standard model handles well. A discharge planner at a hospital refers a patient’s family to your agency. The family Googles your name (branded search), reads 2 reviews on Yelp, visits your website, and then calls. Last-touch credits Google. First-touch credits Google, too, because the referral conversation happened offline with no trackable touchpoint.
The referral, which actually drove the entire conversion, gets 0% credit in every digital model. If your agency has mapped out how each referral gatekeeper makes decisions, you know that the discharge planner’s recommendation carried more weight than all 4 digital touchpoints combined. But your attribution dashboard can’t quantify that weight without manual logging.
Agencies running a marketing diagnostics audit should build a parallel offline attribution log. Every intake coordinator should ask 2 questions: “How did you first hear about us?” and “What made you decide to call today?” Those answers, logged consistently in your CRM alongside the digital trail, create a hybrid attribution picture. It’s imperfect. It relies on self-reported data, which is subject to recency bias (people remember the last thing they saw, not the first). But combined with your digital tracking, it closes the biggest gap in home care lead attribution modeling.
Info: A simple two-question intake script (“How did you first hear about us?” and “What made you decide to call today?”) captures offline referral data that no digital attribution model can track on its own.
What the Data Doesn’t Tell Us
Attribution models assign credit. They don’t explain motivation. A U-shaped model can tell you that organic search and a phone call each deserve 40% of the credit for a conversion, but it can’t tell you that the family chose your agency because a neighbor mentioned your caregiver by name at church. The emotional weight of a personal recommendation, the trust transferred from a physician’s endorsement, the relief a family feels when your website has transparent pricing all live outside the data.
The numbers also can’t account for the timing dynamics specific to senior care decisions. A family that bookmarks your site in January and calls in April after a fall creates a 90-day attribution window. Standard 30-day lookback windows in Google Ads miss that conversion entirely. Extending the window to 90 days captures it but introduces noise, crediting touchpoints from 3 months ago that the family has long forgotten.
What the data does tell you is directional. It tells you that slashing your content budget because blog posts show 0 last-touch conversions is a mistake backed by clear evidence, since 70% of your converters likely touched that content first. It tells you that paid search and retargeting look like heroes because they catch people at the moment of decision, not because they created the demand. And it tells you that tracking home care marketing attribution accurately requires investment in identity resolution, CRM integration, and a willingness to accept that the numbers will always be partially incomplete. The agencies that act on imperfect-but-honest data outperform those chasing a single-channel answer that never existed.


