Families screening senior care providers filter on three credential categories that drive caregiver certification conversion: dementia-specific training, medication management certification, and named-staff qualifications visible on Google Business Profiles and review directories. Generic badges like basic CPR rank low in family decision-making and rarely influence inquiry-to-admission rates.
TL;DR: The credentials that convert families into clients address specific fears (cognitive decline, medication errors, fall risk), appear where families actually research providers, and are tied to individual caregivers by name and photo. Burying certifications on an “About Us” page while hoping families discover them is the single most common trust signal failure in caregiver credentials marketing.
Six rules govern which credentials move families from search to signed service agreement. Each one addresses a different failure point in how agencies present staff qualifications, and each one has a clear exception worth understanding.
Put credentials where families search, not where you’re proud to display them
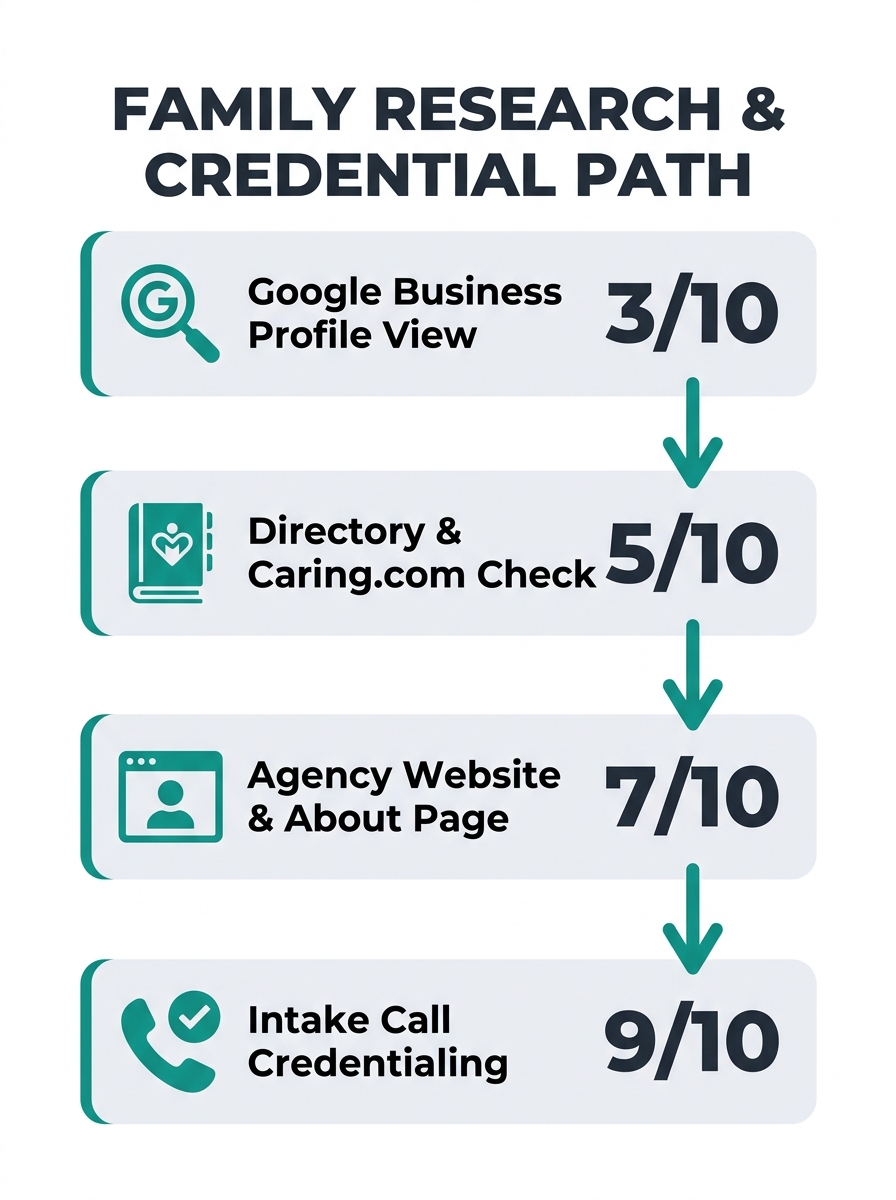
Families evaluate care facilities through a pre-contact filter using Google Business Profile reviews, state inspection reports, and licensing records, according to industry research on care facility credibility and conversion patterns. A credential listed on your website’s team page but absent from your Google Business Profile, your Caring.com listing, and your A Place for Mom directory entry is invisible during the research phase that determines whether families call you at all.
The data backs this up. Consistent name, address, and phone number (NAP) information across all platforms signals credibility to search engines and helps potential clients find your agency. That same consistency principle applies to credentials. If your Google Business Profile description mentions “state-licensed and bonded” but says nothing about dementia training or medication management certification, you’ve wasted the single highest-visibility real estate in your marketing. Our guide to auditing your Google Business Profile for senior care visibility walks through this in detail.
The exception: if your primary lead source is hospital discharge planners or physician referrals rather than organic family search, credential placement on clinical-facing materials (referral packets, discharge coordinator briefs) matters more than directory profiles.
Prioritize dementia and medication certifications over generic training badges
Why does a CPR badge fail to move conversion rates? Because the daughter searching “memory care near me” already assumes basic safety training is in place. Her fear is specific: will this caregiver recognize when Mom’s confusion is a UTI versus sundowning? Will someone double-check medications against the pharmacy list?
The Institute for Healthcare Improvement’s Certified Professional in Age-Friendly Health Care (CPAFH) credential, built on the evidence-based 4Ms Framework (What Matters, Medication, Mentation, and Mobility), directly addresses those anxieties. Organizations like the Center for Caregiver Advancement have built training ecosystems around credential-based advancement, tying dementia care and medication management certifications to measurable position growth.
Certification programs vary from a few days to several weeks and cost anywhere from under $100 to nearly $1,000 depending on state requirements, according to Burd Home Health. The investment pays differently depending on the credential. A dementia care certification displayed prominently converts at a meaningfully higher rate than a generic first-aid badge because it speaks to the condition families are losing sleep over.
| Credential | Family Recognition | Addresses Which Fear | Typical Cost | Conversion Impact |
|---|---|---|---|---|
| Basic CPR/First Aid | Low (assumed baseline) | General safety | Under $100 | Minimal |
| Dementia Care Certification | High | Cognitive decline, wandering | $200–$600 | Strong |
| Medication Management | High | Drug errors, interactions | $150–$500 | Strong |
| Wound Care Certification | Moderate | Post-hospital recovery | $200–$800 | Moderate |
| CPAFH (IHI) | Growing | Age-specific clinical care | $500–$1,000 | Strong for clinical referrals |
| CALA (ACHCA) | Low among families | Administrative competence | Varies by state | Weak for family conversion |
The Certified Assisted Living Administrator (CALA) credential from ACHCA carries institutional weight but doesn’t register with families during their search. It’s an operational credential, valuable for regulatory compliance and professional development. Knowing the difference between credentials that impress peers and credentials that convert families is where most agencies get confused.
Pair every credential with a name and a face
Families look for patterns in reviews that mention specific staff members by name, and they trust those reviews far more than generic praise about “wonderful caregivers.” Research on video messaging shows that people retain 95% of a video message compared to 10% of text, which means a 30-second video introducing “Maria, our dementia-certified care specialist with 8 years of memory care experience” outperforms a bulleted list of agency certifications on your website.
This is the trust signal that separates agencies with identical credential portfolios. When you display certifications at the agency level (“Our team is trained in dementia care”), you’re making an institutional claim. When you display them at the caregiver level (“Your mother’s caregiver, Maria Torres, holds a Level III dementia care certification from the Alzheimer’s Association”), you’re making a personal promise. Families buy the personal promise.
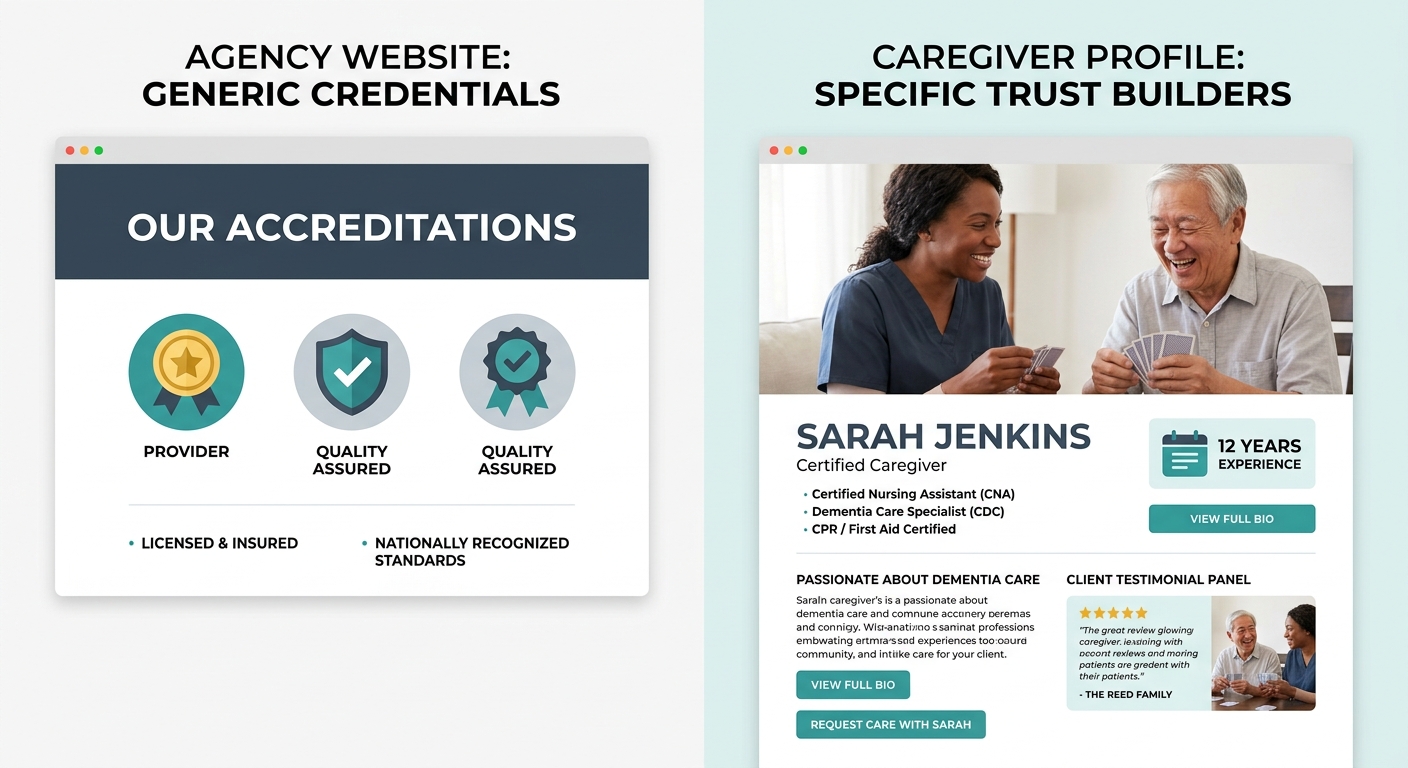
Tip: Add individual caregiver credential spotlights to your Google Business Profile posts. These posts appear in local search results and give families a reason to click through. A monthly “Meet Our Certified Caregivers” post series costs nothing and puts trust signals in senior care directly into the search results page.
Build this into your caregiver career ladder structure so that credential attainment automatically triggers a marketing update. When a caregiver earns a new certification, that achievement should appear on your website, your social profiles, and your directory listings within the same week.
Drop acronyms that families can’t decode
CPAFH. CALA. CNA. HHA. CHHA. The senior care industry runs on alphabet soup that means nothing to a 52-year-old daughter Googling care options at 11 p.m. Every acronym on your marketing materials that requires explanation is a friction point between your care facility credibility and a family’s decision to call.
Write “certified in Alzheimer’s and dementia care” instead of “dementia care certified (DCC).” Write “trained in safe medication administration” instead of “medication management certified.” The credential still exists on the caregiver’s file and in your compliance records. The marketing-facing language needs to be translated into the vocabulary families actually use when they’re afraid.
Every acronym on your marketing materials that requires explanation is a friction point between your credibility and a family’s decision to call.
The exception here is CNA (Certified Nursing Assistant), which has enough public recognition to use without translation. Test the rest by asking someone outside the industry what each acronym means. If they can’t answer in 5 seconds, spell it out.
Match credential messaging to the specific fear driving the inquiry
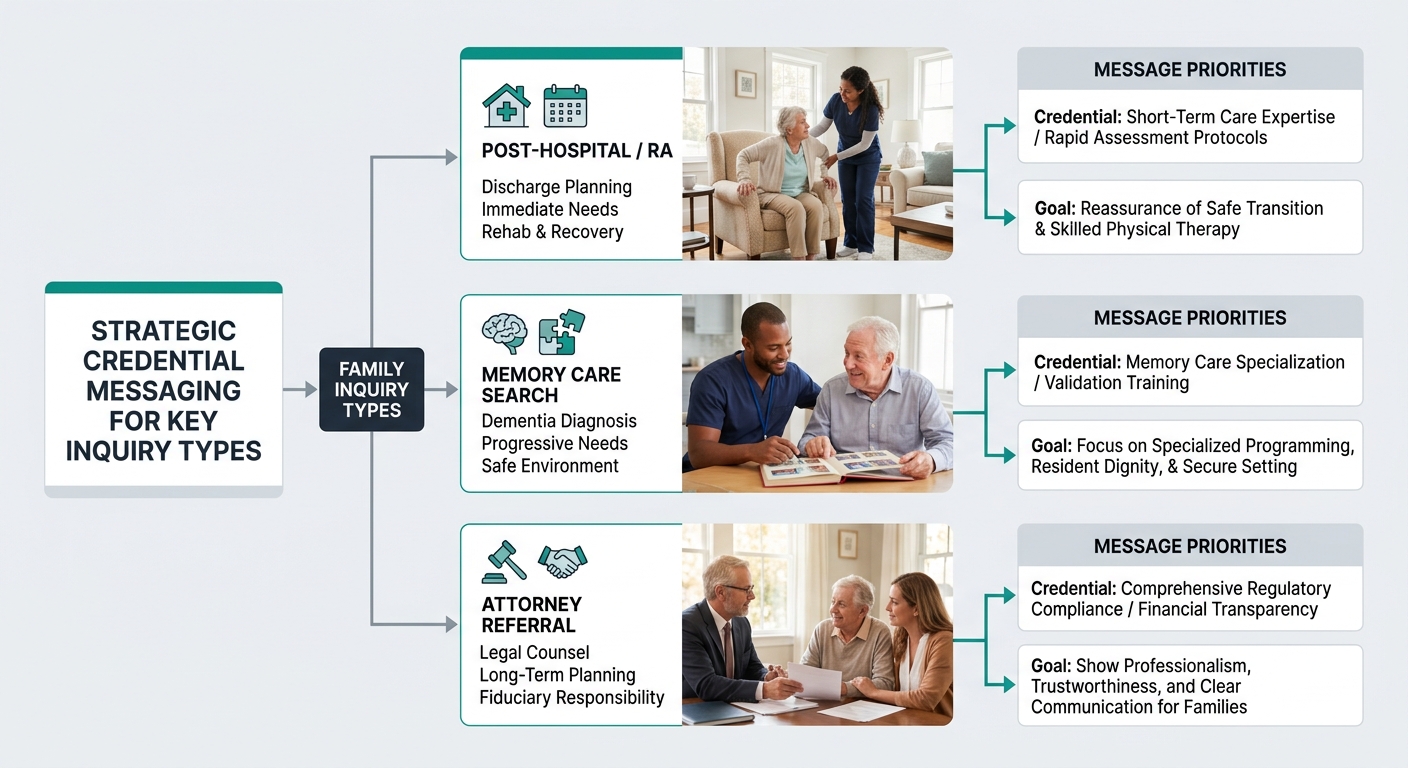
As HealthLeaders Media reported, integrated family care models stress “partnership with families and a continual effort to be responsive to their needs”. That responsiveness starts before intake. The credential you lead with should change based on the inquiry source and the concern expressed.
A family calling after a hospital discharge cares about wound care training and medication management. A family researching memory care options over weeks cares about dementia-specific qualifications and behavioral management experience. A family referred by an elder law attorney cares about compliance credentials and liability coverage. Your intake team should have 3 different credential talking points ready depending on which fear is driving the conversation, and your marketing materials targeting different decision-makers in the family should reflect those same distinctions.
Agency representatives who can educate clients on specific caregiving-related concerns during the intake process improve start-of-care rates. The credential becomes the proof point behind the education, not a line item on a brochure.
Audit what your referral partners actually say about your staff
Community-based client acquisition works best when in-person local engagement and digital channels reinforce each other. But there’s a gap most agencies never check: what do your referral partners actually tell families about your caregivers’ qualifications?
Call 3 of your top referral sources this week and ask a direct question: “When you recommend us, what do you say about our staff’s training?” If they can’t name a single specific credential, your referral marketing has a trust signal leak. Discharge planners, social workers, and geriatric care managers need a one-sentence credential summary they can repeat without looking it up. “Their caregivers are all dementia-certified and medication-trained” is repeatable. “They’re a great agency” is not.
This connects to your broader reputation management for home care strategy. Online reviews, referral partner language, and your own marketing materials should all echo the same specific credential claims. When a family hears “dementia-certified” from their social worker, sees it in your Google reviews, and reads it on your website profile, the repetition builds the kind of layered trust that converts. One bad experience with a phone receptionist who can’t speak to caregiver qualifications can undo that entire chain, so train your intake staff on the same credential vocabulary you train your referral partners on.
Warning: If your video testimonials feature families praising “wonderful care” without mentioning specific training or qualifications, you’re collecting social proof that doesn’t reinforce your credential story. Our breakdown of [conversion elements in senior care video testimonials](/blog/video-testimonials-conversion-elements-senior-care) covers how to prompt for specificity.
When These Rules Collapse
These six rules assume your primary conversion channel involves families who research before they call. And for most home care agencies and assisted living communities, that assumption holds. But some agencies operate almost entirely on hospital discharge referrals with 24-to-48-hour decision windows. In that environment, credential marketing shifts from consumer-facing trust signals to clinical shorthand that discharge coordinators recognize instantly. The CPAFH and CNA acronyms you’d normally spell out become speed signals for a case manager triaging 15 discharge orders before lunch.
The other collapse point is geographic. Rural markets with 1 or 2 provider options see less credential comparison because families have fewer choices. In those markets, availability and proximity override credential display. Your trust signals in senior care still matter for retention and referral generation, but they carry less weight in the initial conversion moment when the alternative is no care at all. Knowing which environment you operate in determines how much of your marketing budget should go toward credential visibility versus capacity messaging. The audit still matters. You’re just reading the results through a different lens.


