Home care referral mapping assigns every hospital discharge planner, hospice, skilled nursing facility, and geriatric care manager in your service area to a specific outreach rep with a defined visit cadence and conversion target. The common alternative, dropping brochures at every facility within driving distance, scatters your outreach hours across sources that will never send you a qualified client.
TL;DR: Territory mapping treats your referral network like a sales territory: segmented by clinical opportunity, assigned to individual reps, tracked in your CRM, and measured by actual intake conversions rather than facility visits logged.
How Territory Mapping Differs from a Contact List
Most agencies maintain some kind of referral contact spreadsheet. A territory map is a fundamentally different tool. Where a contact list records names and phone numbers, a territory map layers in referral volume potential, geographic proximity to your caregivers, payer mix, facility discharge rates, and competitive saturation. Each referral source gets scored and assigned to a rep who owns that relationship.
The distinction matters because home care operates with a 79.2% annual client turnover rate, according to Home Care Pulse benchmarking data. At that churn rate, you need constant inflow of new referrals to maintain census. A contact list doesn’t tell you which 15 of your 80 contacts actually generate volume. A territory map does, because it tracks conversion data alongside relationship activity.
Modern territory planning in healthcare sales, as Alpha Sophia’s 2026 analysis describes it, “divides markets into balanced, executable territories based on clinical opportunity, not geography alone.” That principle applies directly to home care outreach. Your territory boundaries should reflect where clinical need concentrates, not where the nearest highway exit happens to be.
Segmenting Your Total Addressable Market
Why start with your total addressable market instead of your existing contacts? Because the contacts you already know represent a fraction of the available opportunity. The first step, as Definitive Healthcare outlines in their guide to healthcare sales territories, is to analyze your TAM and segment it into logical groups using criteria like geographic location, facility size, payer mix, and discharge volume.
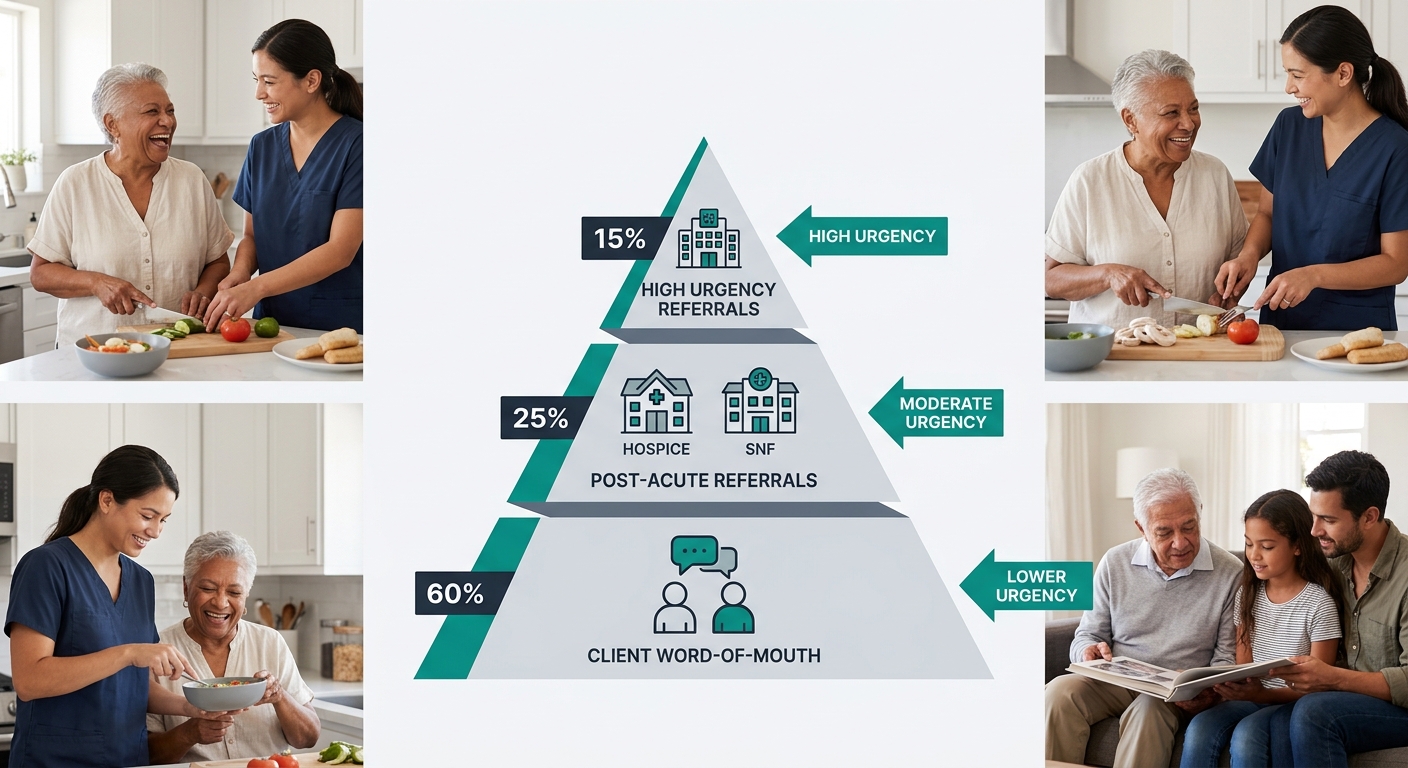
For home care, benchmarking data breaks down where referrals actually originate:
| Referral Source | Share of All Referrals | Typical Urgency |
|---|---|---|
| Current and past clients | 19.5% | Low (relationship-driven) |
| Hospital discharge planners | 8.8% | High (48-72 hour window) |
| Medicare-certified home health agencies | 7.1% | Medium |
| Skilled nursing facilities | 5.9% | Medium-high |
| State Medicaid waiver programs | 5.7% | Variable |
| Hospice providers | 5.1% | High |
| Geriatric care managers | 4.2% | Medium |
| Area Agencies on Aging | 4.0% | Medium-low |
These numbers reveal a critical pattern: no single source dominates. Your highest-volume channel (past and current clients at 19.5%) still accounts for fewer than 1 in 5 referrals. That fragmentation is exactly why a territory-based marketing strategy matters. You can’t afford to ignore any category, and you can’t afford to treat them all the same.
Shelle Womble of corecubed, a home care marketing consultancy, recommends that agencies maintain “at least 20 solid referral sources” to avoid dangerous over-reliance on any single channel. She notes that medical community partners like home health agencies, hospice providers, and assisted living facilities qualify as “low hanging fruit” because their referrals are typically “vetted and in immediate need of care.”
The Four-Variable Source Score
Once you’ve cataloged your sources, each one needs a score. Agencies that build effective client-source attribution systems can pull this data directly from their CRM. If you’re starting from scratch, build your scoring model around four variables:
- Referral volume potential (estimated discharges or client contacts per month)
- Payer mix alignment (does this source send clients whose payer types you accept?)
- Competitive saturation (how many other agencies already call on this source?)
- Geographic fit (can your existing caregiver pool actually serve clients from this source?)
A hospital with 400 monthly discharges but 3 competing agencies already embedded in its discharge planning office scores differently than a hospice with 50 monthly patients and zero existing home care partnerships. The hospice might be your higher-priority target despite lower raw volume, because your conversion rate will be dramatically higher without entrenched competition.
Tools like PowerMaps from Homecare Boost add demographic overlays including age distribution, income levels, veteran populations, and private pay potential. Agencies serving VA home care benefit clients, for example, can filter for veteran population density and focus hospital partnership outreach on VA medical centers and affiliated clinics. Agencies targeting private pay can identify zip codes where median household income exceeds $75,000 and concentrate referral source identification in those areas.
Rep Assignments and Visit Cadence
Territory balance is the difference between a system that sustains itself and one that burns out your best marketer. Each rep’s territory should contain a roughly equal mix of high-potential and maintenance-level sources, with visit cadences matched to source priority.
A reasonable framework for visit frequency:
- Tier 1 sources (top 20% by referral volume): weekly in-person visits
- Tier 2 sources (middle 40%): biweekly visits with phone check-ins between
- Tier 3 sources (bottom 40%): monthly visits, supplemented by home care email campaigns that keep your agency visible between face-to-face contacts
This tiered structure prevents the common trap where reps spend equal time on a geriatric care manager who sends 8 referrals per month and a senior center that sends 1. According to a guide on referral strategies from Brasstacks, the key to sustainable referral growth lies in “consistency, structured outreach, measurable KPIs, and empowered teams.”
No single referral source accounts for more than 19.5% of total volume. The fragmentation of referral channels is exactly why you need a mapped system, not a favorite contact.
When you’re identifying the right decision-makers at each facility, remember that the person with the title “discharge planner” isn’t always the person who actually hands families a list of home care options. Social workers, case managers, and floor nurses all influence referral flow. Your territory map should track the functional decision-maker at each source, not the organizational chart title.
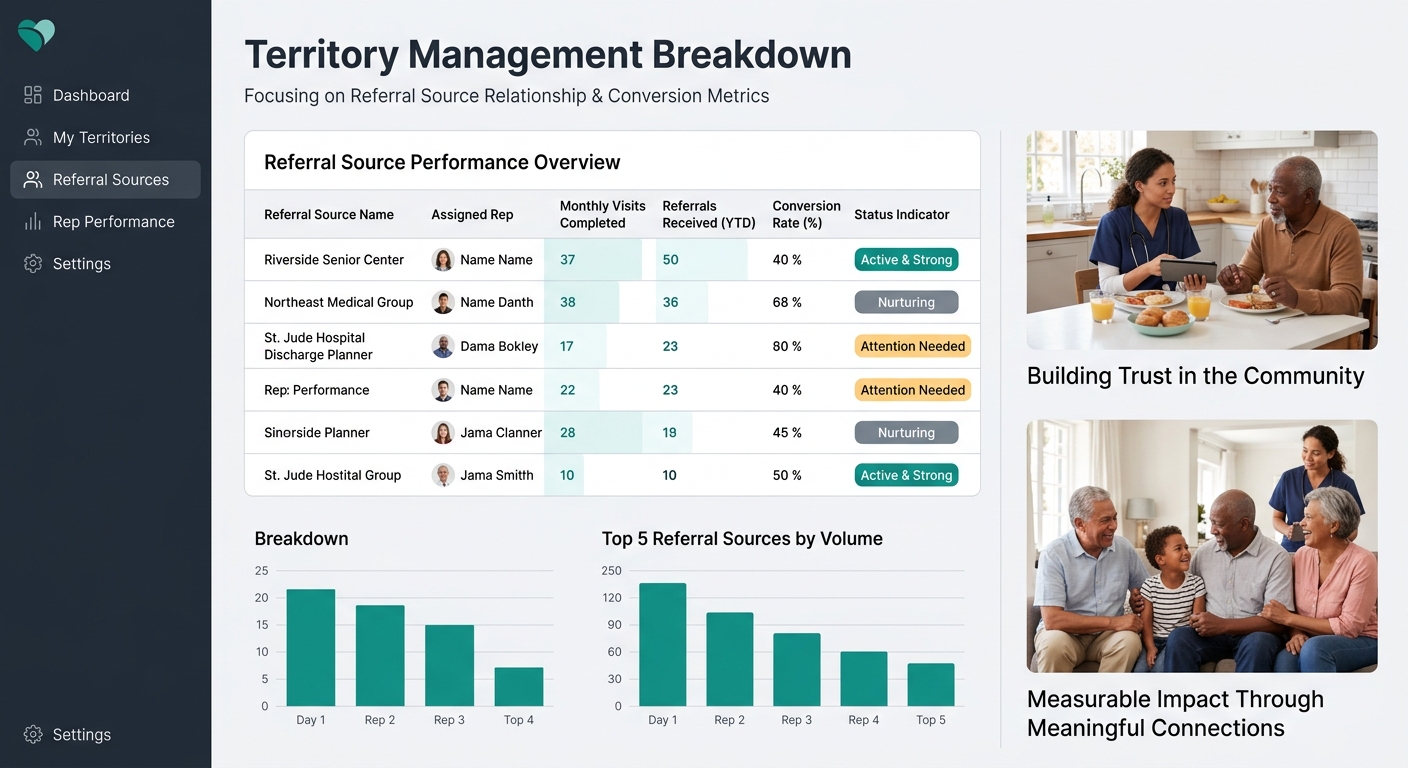
CRM Tracking That Connects Visits to Intake
A territory map without measurement is a wish list. Your CRM should connect three data streams: outreach activity (who visited which source and when), referral volume (how many referrals arrived from each source per period), and intake conversion (how many of those referrals became paying clients).
With structured data, agencies can identify their most valuable referral sources, allocate marketing time wisely, and improve intake performance. The math is straightforward: if Rep A visits Hospital X 4 times per month and generates 6 referrals that convert at 50%, that source produces 3 new clients monthly. If Rep B visits Hospice Y 4 times per month and generates 2 referrals that convert at 90%, Hospice Y produces 1.8 new clients monthly. Both sources matter, but your territory scoring should reflect these different conversion profiles when you reallocate time next quarter.
Nielsen research shows 92% of consumers trust recommendations from people they know above all other forms of advertising. That number explains why relationship depth with referral sources correlates so strongly with conversion rates. A discharge planner who knows your intake coordinator by name and trusts your agency’s reliability will send warmer referrals that close at higher rates than cold inquiries from a source you visited once.
Build your tracking to flag when visit frequency drops below the target cadence. If a Tier 1 source hasn’t received a visit in 10 or more days, your system should surface that gap automatically, not wait until monthly reporting reveals a referral dip you could have prevented.
Where the Model Breaks
Territory mapping fails in three predictable ways. Understanding these failure points prevents you from abandoning a good system when it hits normal friction.
Turnover at the source level. Hospital discharge planners change roles frequently. When hospitals face severe staffing shortages or reorganize departments, your carefully mapped relationships reset to zero. Build redundancy by knowing at least 2 contacts per facility instead of relying on a single champion. The PMC’s research on hospital and public health partnerships identified 8 core characteristics and 11 evidence-based recommendations for successful partnerships, and nearly all of them emphasized institutional relationships over individual ones.
Rep turnover inside your own agency. When a community liaison leaves, every relationship in their territory goes cold overnight. Documenting relationship history in your CRM (not in the rep’s personal notebook) protects against this. The territory belongs to the agency, not the person who drove the route.
Confusing activity with results. Twelve visits per week means nothing if zero referrals follow. Agencies that invest in review management for care agencies and track referral-to-intake conversion can distinguish between reps who build productive relationships and reps who are logging windshield time. Without conversion tracking, territory mapping becomes an expensive scheduling exercise that looks productive on paper while census stagnates.
The system also strains when agencies expand outreach into new geographies before establishing sufficient caregiver density to serve the referrals they generate. A territory map that produces 15 referrals per month from a zip code where you have 2 available caregivers creates a service delivery problem that damages the very relationships you built. Match your outreach ambitions to your actual staffing capacity, especially given the industry-wide staffing shortfalls that constrain caregiver availability across most markets. A territory map is a precision tool. Precision requires honesty about what you can actually deliver when the referrals start arriving.


