Home care agencies lose roughly 30% of potential referral conversions due to communication failures that happen within the first 30 days after a promising introductory meeting with a discharge planner or physician office. The five most damaging post-meeting mistakes each follow a predictable pattern, and each is recoverable if the agency catches it within a specific window.
The Thank-You That Never Arrived (or Arrived Wrong)
The single highest-impact action after a first meeting with a referral source takes fewer than five minutes. According to the Home Care Marketing & Management blog, agencies should “send a personal message or make a phone call, updating them on the status of the lead” every time a referral source sends a patient their way. The same principle applies to the relationship itself after that introductory sit-down.
And yet, the most common failure is the simplest one: the agency sends no follow-up within 48 hours, or sends a generic “great to meet you” message that could have been addressed to anyone at any facility. Discharge planners evaluate three to five agencies simultaneously when building their referral lists. The agency that sends a personalized note referencing a specific pain point discussed in the meeting lands on the short list. The agency that sends nothing, or sends a form email, disappears from consideration.
The recovery window here is narrow but forgiving. If you missed the 48-hour mark, send a handwritten note within the first week. Reference something specific from the conversation: the planner’s frustration with missed pickups, the weekend coverage gap they mentioned, the particular patient population they serve. Specificity signals that you were listening, which is the entire point of the first meeting.

When you’re tracking these touchpoints, the infrastructure matters. Agencies that use a dedicated referral partner portal versus a standard CRM can automate follow-up reminders without losing the personal feel, because the system logs the meeting context alongside the contact record. A reminder that says “follow up with St. Mary’s” is useless if nobody remembers what was discussed.
The Template Blast That Erased the Personal Connection
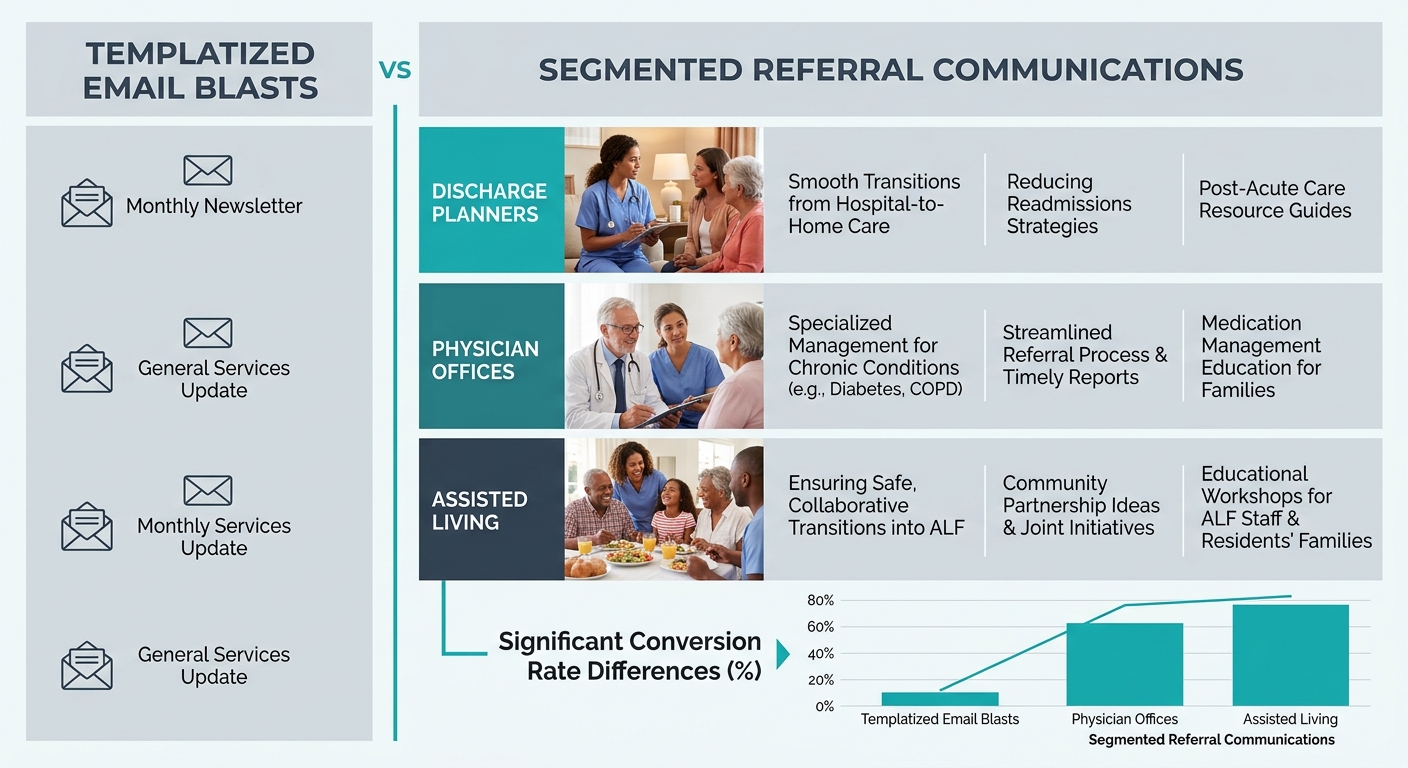
HCMP’s referral marketing guidance is blunt on this point: agencies should “send a thoughtful, personalized email, not a templatized blast” when communicating with potential referral partners. The instruction specifically says to “address the email to a specific person” and tell them “who you are, what your agency offers, and the scope of your service area.”
Here’s where the second mistake compounds the first. An agency has a good first meeting with a discharge planner at a rehab facility. Two weeks later, that planner starts receiving the agency’s monthly e-newsletter, bulk-sent to 400 contacts, featuring stock photos and generic wellness tips. The planner sees the same email that went to every physician office, assisted living community, and elder law attorney in the county. The personal relationship the agency built in person dissolves into marketing noise.
The math on this is painful. Referral clients convert three times faster and carry 60% to 80% lower acquisition costs than paid leads, according to industry referral tracking data. Every templatized blast that alienates a discharge planner or physician office effectively triples the cost of acquiring the clients that planner would have sent you.
Recovery requires segmentation. Pull your referral contacts out of your general marketing list immediately. Build a separate communication track for each referral source category: discharge planners get clinical outcome updates and case study summaries. Physician offices get patient progress reports. Assisted living communities get information about complementary services. If you’re running email marketing for care providers, the segmentation is where your referral ROI lives or dies.
Silence Where a Status Update Should Have Been
The third mistake is the one that burns the most bridges, and it’s the one agencies are least aware they’re making. Data from referral management studies shows that 63% of referring physicians express dissatisfaction with the communication they receive after referring a patient to another provider. The complaint is consistent: they send a patient, and they hear nothing back about what happened.
For home care agencies, this looks like a discharge planner who refers a patient for post-surgical care, and then gets no confirmation that the intake happened, no update on the care plan, and no notification when the patient’s needs change. The planner has to call the agency, wait on hold, and ask for information they should have received automatically.
The research from Home Care Sales on discharge planner outreach highlights “regular check-ins” as essential to “reinforce relationships and keep the agency top-of-mind.” But check-ins about the relationship are secondary to check-ins about the patient. The referral source wants to know their patient is being served. That’s the closed loop that generates the next referral.
Recovering from a communication gap requires a concrete change in workflow, not an apology. Build a status update protocol: within 24 hours of intake, the referral source receives confirmation that the patient was accepted and a summary of the initial care plan. At 7 days, they get a brief progress note. At 30 days, a milestone check-in. Agencies that build a client-source attribution system can track which referral sources are receiving these updates and which are falling through the cracks.
Tip: If you’ve gone silent on a referral source for more than two weeks after they sent you a patient, call them directly. Don’t email. A phone call signals urgency and respect. Update them on the patient’s status and tell them exactly what your communication cadence will look like going forward.
The Referral Packet That Answered the Wrong Questions
LeadSquared’s guide to home care referral sources recommends agencies “create concise referral packets with service details and contact info.” Concise is the operative word. The fourth mistake agencies make is handing a discharge planner a 12-page folder full of company history, mission statements, caregiver bios, and testimonial pages that answer none of the questions the planner actually has.
Discharge planners need to know four things: what geographic area you cover, what hours you staff (including weekends and holidays), what services you can start within 24 to 48 hours of referral, and who to call when something goes wrong at 2 AM. Research on physician referral networks from ReferralMD identifies “incomplete understanding” of care capabilities as a core driver of referral breakdowns. If your packet doesn’t answer the planner’s operational questions on a single page, the rest of the material is padding.
The recovery here is straightforward: redesign the packet around the referral source’s workflow. Create a one-page quick-reference sheet with your service area map, after-hours contact number, average intake-to-start time, and the three most common diagnoses your caregivers handle. Put everything else in a digital follow-up. Healthcare Success’s research on referral-building mistakes notes that physicians who show “lack of professional respect for their staff, or for the staff at the referring office, are wearing down the practice-to-practice relationship.” An overwhelming, irrelevant packet communicates the same disrespect: you didn’t bother to learn what the planner needs.
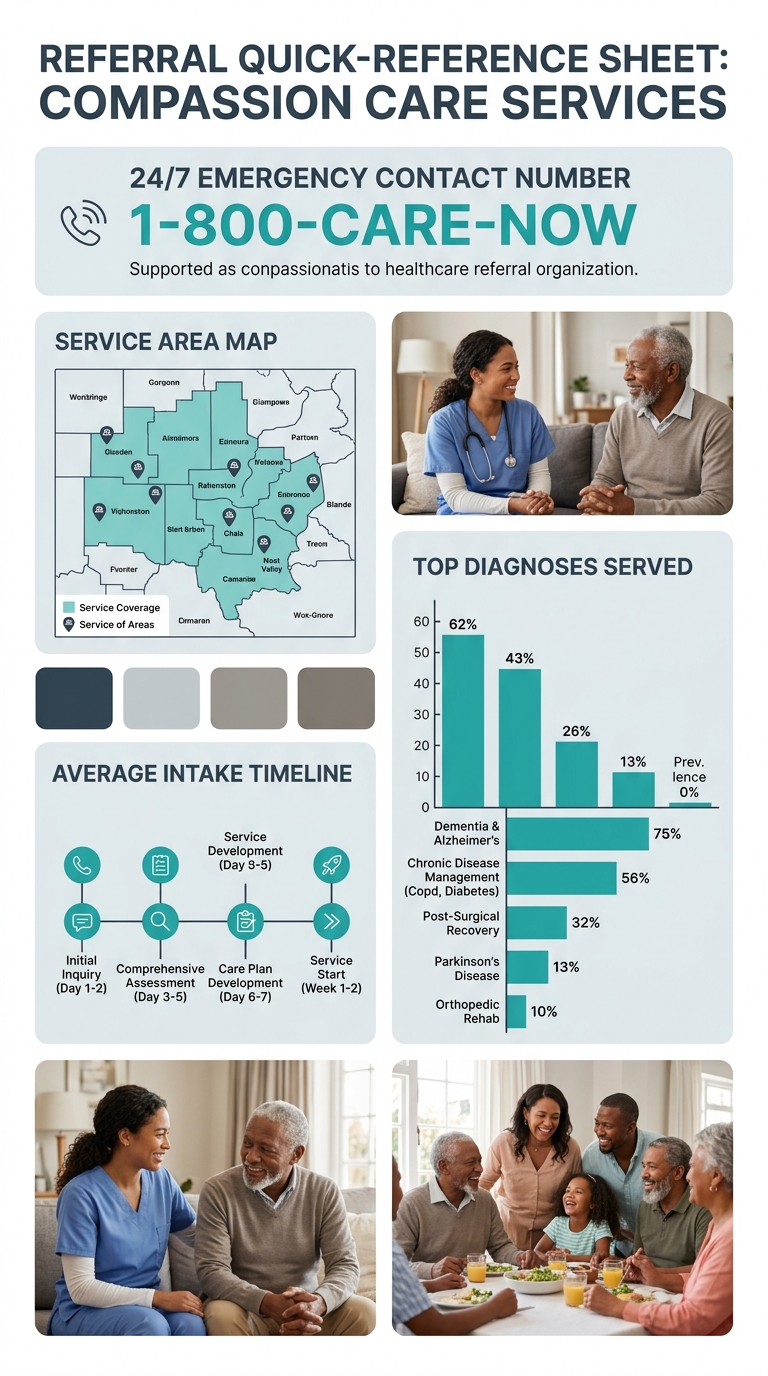
If you’ve already distributed an unwieldy packet, send the updated one-pager with a brief note: “We realized our original materials didn’t make it easy to reach us when you need to. This is the only page you need.” That kind of honesty strengthens the relationship rather than weakening it. And make sure your referral source territory map is current so the geographic coverage information on that one-pager is accurate down to the zip code.
Nine Weeks Out and the Relationship Has Gone Cold
The fifth mistake is the slow fade. The first meeting went well. Maybe the agency even avoided mistakes one through four. But by week six, the check-in calls stopped. By week nine, the discharge planner has moved on to an agency that showed up consistently. Industry data shows that structured follow-ups, including “satisfaction surveys, milestone check-ins, and share-your-story campaigns,” directly convert gratitude into measurable referral growth. Agencies that don’t systematize this cadence lose referral sources to competitors who do.
The cost is measurable. When you consider that referral clients carry acquisition costs 60% to 80% lower than paid leads and convert three times faster, a single lost discharge planner relationship can represent tens of thousands of dollars in annual revenue. An agency serving a mid-size market with four hospital systems might maintain relationships with 15 to 20 discharge planners. Losing three of them to the slow fade is the equivalent of cutting your most profitable marketing channel by 15% to 20%.
A single lost discharge planner relationship can represent tens of thousands of dollars in annual revenue. And most agencies don’t even realize it’s gone until the referrals stop.
Recovery from a cold relationship takes more than a phone call. It takes something worth calling about. Bring a specific, relevant update: a new service line you’ve added, a weekend staffing expansion, a case outcome that demonstrates your agency’s reliability. Reference the original conversation from your first meeting. Show that the relationship has continuity, even if you let it lapse.
Building this kind of consistency into your agency’s operations requires accountability at the management level. Track referral source contact frequency the same way you track caregiver hours and client satisfaction. Agencies that invest in reputation management for home care often find that the same systems that monitor online reviews can surface referral relationship gaps: if a hospital system that used to send you four referrals a month drops to zero, that’s a signal to investigate before the relationship is truly lost.
The pattern across all five mistakes is the same. Agencies invest real time and energy into earning the first meeting with a discharge planner, physician office, or senior living community. They prepare talking points, bring branded materials, and show up with genuine enthusiasm for the partnership. Then the follow-through collapses because nobody owns the post-meeting relationship. The first meeting is a marketing event. Everything after it is an operations problem, and agencies that treat it as such convert referral meetings into referral revenue at dramatically higher rates than those still waiting for the phone to ring.


