Referral marketing and relationship marketing operate through different mechanics, reward different behaviors, and produce different pipeline outcomes. Senior care operators routinely treat them as synonyms, running relationship-building activities while expecting referral-volume results. That confusion drains admissions budgets and stalls census growth across home care, assisted living, and skilled nursing.
TL;DR: Referral marketing is a structured acquisition channel with incentives, tracking, and measurable conversions. Relationship marketing is a long-term engagement strategy focused on retention and trust. Operators who conflate the two measure neither properly, lose ground on both, and blame “networking” when census dips.
Two Systems Running on Different Fuel
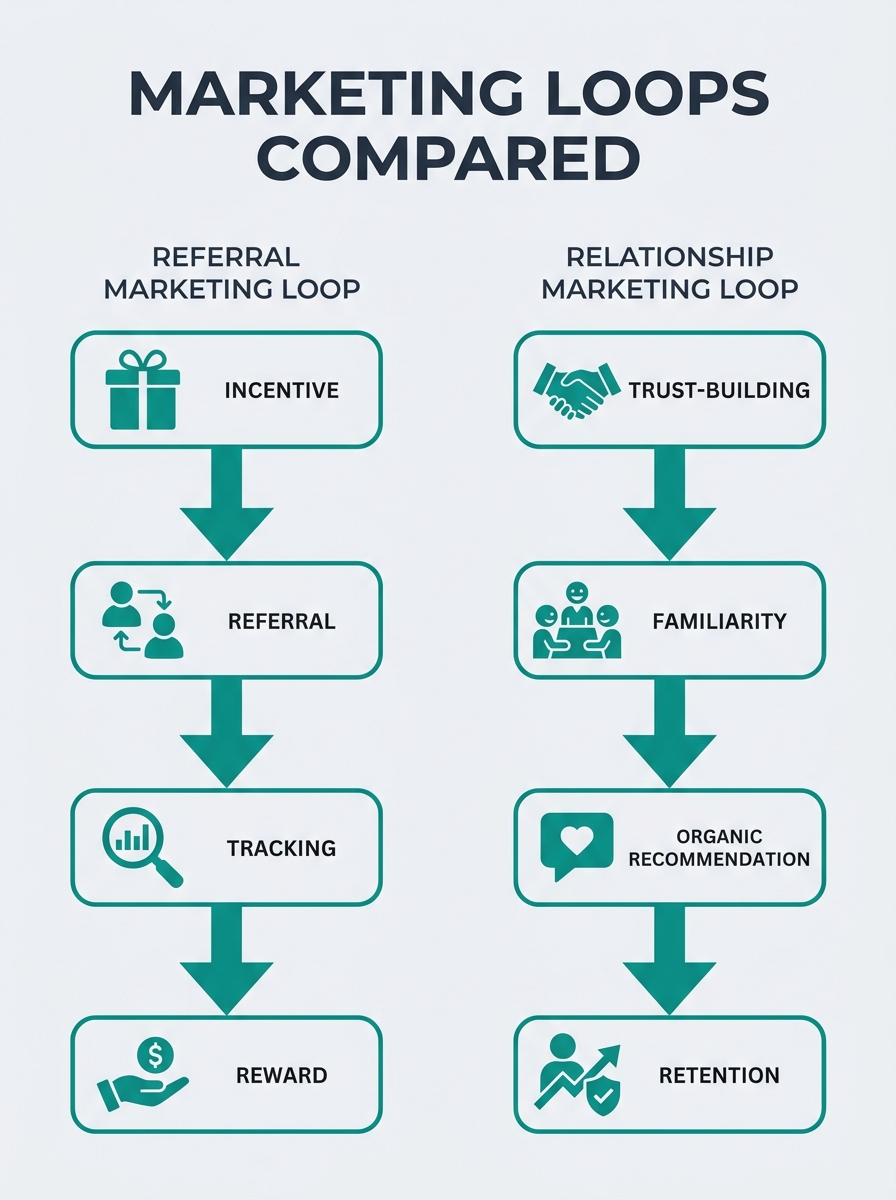
Referral marketing actively incentivizes and rewards existing customers for referring new ones, allowing the organization to influence, track, and measure each referral event. The fuel is transactional: someone sends a qualified lead, the outcome gets tracked, and the referring party receives acknowledgment, a reward, or both. The cycle is short. You can count it in days or weeks.
Relationship marketing runs on a different compound entirely. As GrowSurf’s referral marketing glossary defines it, relationship marketing focuses on long-term goals with a person rather than short-term actions. The timeline stretches across months and years. You’re building trust, deepening familiarity, and positioning your organization as the default recommendation when someone asks a discharge planner or elder law attorney where to send a patient.
Both systems produce leads. The confusion starts because operators see leads arriving from professional contacts and assume the same activity generated them, whether that activity was a structured referral ask or a quarterly lunch.
The following table illustrates the mechanical difference between these systems, along with what operators typically end up doing when the two blur together:
| Attribute | Referral Marketing | Relationship Marketing | What Operators Actually Do |
|---|---|---|---|
| Primary goal | Generate tracked, attributable leads | Build long-term trust and loyalty | “Get more referrals” (undefined) |
| Timeline | Days to weeks per cycle | Months to years | Sporadic, event-driven |
| Tracking | CRM-logged per referral source | Satisfaction surveys, NPS, retention rates | Anecdotal (“Dr. Kim sends us patients”) |
| Core activity | Structured asks, incentive programs, referral portals | Newsletters, community events, ongoing touchpoints | Lunch drop-offs and holiday cards |
| Key metric | Referral-to-admission conversion rate | Client lifetime value, retention rate | “Number of contacts made this month” |
| Fuel | Incentives, recognition, ease of referral process | Consistent value delivery over time | Good intentions |
The Anatomy of a Senior Care Referral Marketing System
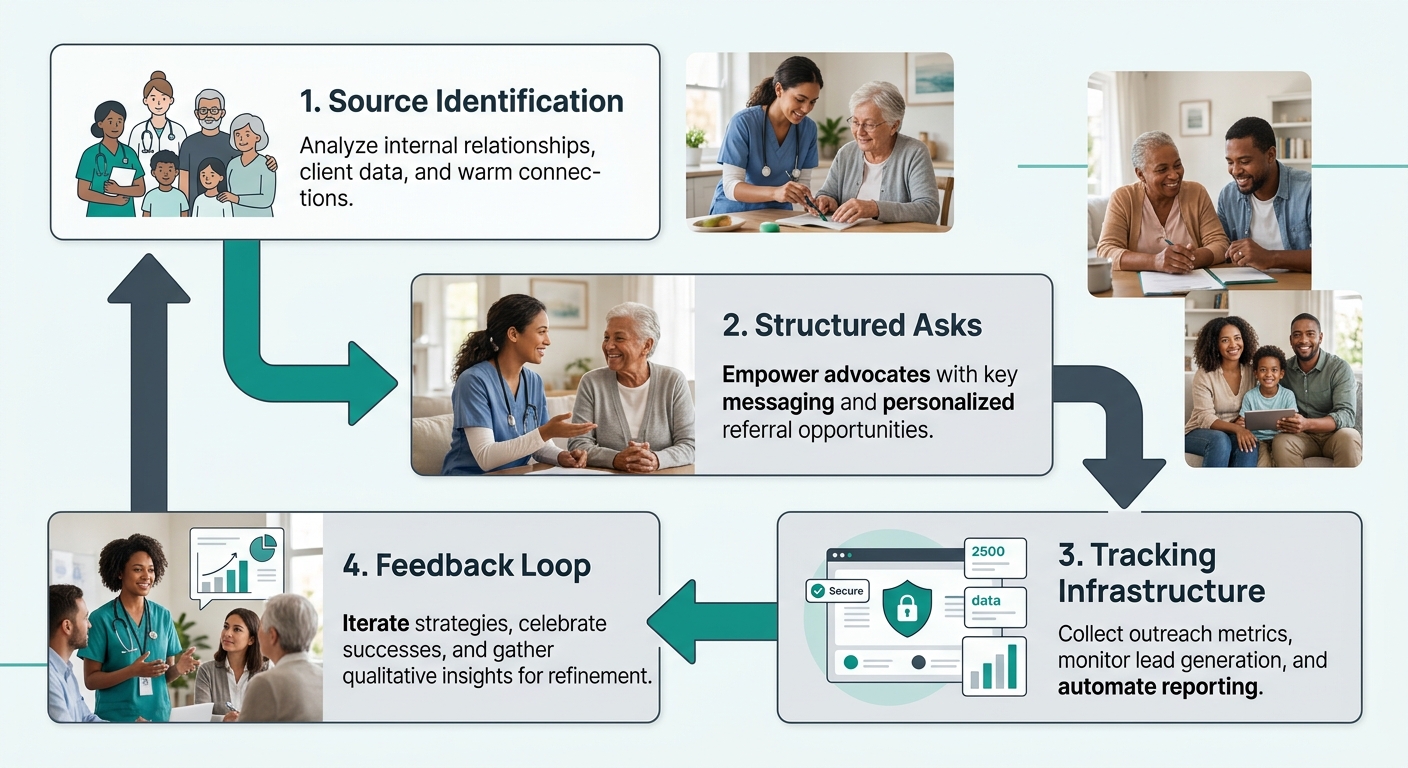
A real home care referral marketing system has four moving parts: source identification, structured asks, tracking infrastructure, and a feedback loop. Remove any one, and you’re back to relationship marketing wearing a referral marketing label.
Source identification starts with data. NIC MAP’s guidance to senior housing operators names the specific professional categories worth cultivating: social services personnel, discharge planners, and facility case managers are the high-yield targets. Friends and family referrals also contribute volume, but the professional channel tends to deliver prospects further along in the decision process. If you’ve ever mapped your referral source territory, you know that not every contact on your list produces admissions at the same rate.
Structured asks are where most senior care operators stumble. A structured ask has a clear trigger (“When you discharge a patient who needs 20+ hours of home care per week, here’s exactly how to refer them to us”), a defined process (referral form, portal login, direct phone line), and a reason for the source to choose you over the 4 other agencies who also dropped off brochures. Without these three components, your “referral source development” is actually relationship maintenance.
Tracking infrastructure connects each incoming lead to its source. Agencies that rely on “How did you hear about us?” intake questions lose attribution accuracy fast. A dedicated referral partner portal or CRM system designed for source tracking closes that gap by logging every referral against the professional who sent it, the date, and the outcome.
The feedback loop is the piece that makes the system self-reinforcing. When a discharge planner sends you a patient and hears nothing for 6 weeks, that planner stops sending. When they receive a same-day acknowledgment, a 7-day update on the patient’s care plan, and a quarterly summary of how many of their referrals converted to active clients, the relationship deepens because it’s grounded in measurable outcomes.
Where Relationship Marketing Belongs in Senior Care
None of this means relationship marketing is unimportant. It serves a distinct purpose: keeping your organization top of mind among people who aren’t ready to refer today but will encounter referral opportunities over months and years. Community engagement, as research from senior living providers emphasizes, significantly impacts the well-being of elderly residents and the perception of the community among outside professionals.
Your Alzheimer’s education seminar at the local library is relationship marketing. Your monthly email newsletter to case managers sharing clinical insights is relationship marketing. Your sponsorship of the hospital’s annual gala is relationship marketing. These activities build familiarity and trust. They warm the soil.
But they don’t plant seeds with specific germination dates. And they don’t track which seed grew into which admission.
The problem emerges when operators invest 80% or more of their community marketing budget in relationship activities and then wonder why they can’t tie any specific investment to a specific admission. The answer is straightforward: relationship marketing wasn’t designed to produce that kind of attribution. You’re asking a thermometer to tell you the time.
You’re asking a thermometer to tell you the time. Relationship marketing wasn’t designed to produce referral attribution, and blaming it for failing at that job misses the point entirely.
How Operators Cross the Wires
The conflation happens for three reasons that tend to reinforce each other inside senior care organizations.
First, the same person often does both jobs. A community liaison at an assisted living community or a marketer at a home care agency handles relationship maintenance (lunches, event invitations, check-in calls) and referral generation (structured asks, portal setup, conversion tracking) as a single role. When the job description doesn’t distinguish between the two, the reporting doesn’t either. Activities get logged as “outreach contacts” regardless of whether the contact was a trust-building touchpoint or a referral solicitation. As NIC MAP advises, operators should “use a variety of outbound marketing strategies that includes online outreach as well as in-person visits, phone calls, and even hand-written cards of thanks when warranted,” but variety without categorization produces measurement fog.
Second, CRM systems in senior care rarely enforce the distinction. If your contact log records “met with Dr. Patel” without tagging whether the meeting included a structured referral ask, a portal enrollment, or a conversion discussion, you’ve captured activity without capturing intent. Agencies that have built a proper client-source attribution system can separate these two streams. Agencies without one treat every logged contact as evidence that referral marketing is happening.
Third, the word “referral” itself causes damage. In senior care, “referral” gets used to describe everything from a hospital discharge planner sending a patient with specific care needs and insurance documentation to a neighbor mentioning your community’s name at a dinner party. These are categorically different events with different conversion probabilities, different follow-up protocols, and different costs to generate. Lumping them under one word makes it impossible to budget accurately for either.
Info: When your team logs “referral contacts” without distinguishing between relationship touches and structured referral asks, you lose the ability to calculate cost-per-referral or referral-to-admission conversion rate for either channel.
Professional Sources Need a Different Protocol Than Family Sources
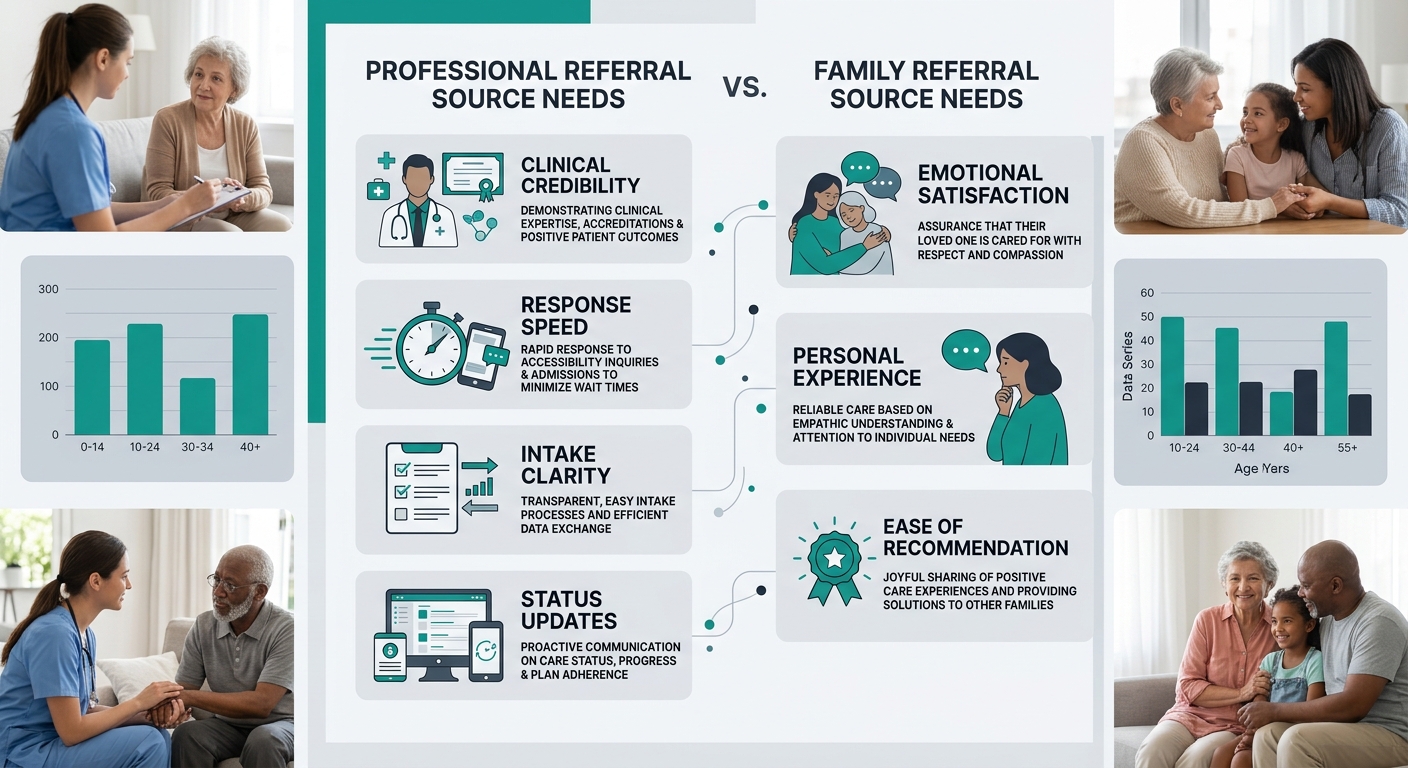
Why does the distinction between referral vs relationship marketing matter at the tactical level? Because professional referral sources and family referral sources respond to completely different signals.
Discharge planners and social workers need clinical credibility, fast response times, and clear intake processes. They send patients to agencies that make their job easier, reduce readmission risk, and communicate status updates without being chased. For professionals in nursing home marketing and home care alike, the referral system must feel frictionless on the source’s end. A discharge planner managing 30+ cases per month won’t tolerate a referral process that requires a phone call, a voicemail, and a callback.
Family referral sources operate differently. A daughter who recommends your agency to a coworker does so based on emotional experience: how her mother was treated, how responsive the office was when she called worried, whether she felt informed and respected. That recommendation happens organically, driven by the relationship marketing you’ve invested in. You can encourage it with a structured program (referral cards, small thank-you gestures, follow-up calls asking if they know anyone who could benefit from care), but the initial impulse comes from satisfaction, not from incentives.
Operators who have avoided the common mistakes that derail referral source relationships after the first meeting understand this split intuitively. The protocol for maintaining and converting a professional source looks nothing like the protocol for encouraging organic family recommendations. Treating them identically guarantees underperformance in both channels.
The Tradeoffs Nobody Budgets For
Separating referral marketing from relationship marketing forces uncomfortable budget conversations. A proper home care referral marketing system requires CRM investment, portal infrastructure, staff time dedicated specifically to structured asks and conversion tracking, and incentive programs with real costs attached. Relationship marketing requires consistent content production, event budgets, community presence, and long-horizon patience without clean ROI attribution.
Most senior care operators can’t fully fund both simultaneously. The tradeoff is real: invest heavily in referral marketing infrastructure and you’ll see faster, more attributable admissions growth, but you’ll underinvest in the trust-building that keeps your reputation warm across the broader community. Invest heavily in relationship marketing and you’ll be well-liked, well-known, and unable to explain to your board why 60% of your admissions came from channels you can’t trace.
The honest answer is that a senior care referral strategy needs both, but in clearly labeled budget lines with separate KPIs. Relationship marketing gets measured by NPS, retention rate, community awareness, and event attendance. Referral marketing gets measured by referral-to-tour conversion, tour-to-admission conversion, cost per referral, and source-specific volume trends.
When operators stop conflating these two systems, something useful happens: they stop blaming relationship investments for failing to produce referral metrics, and they stop expecting referral infrastructure to generate the kind of broad community goodwill that only comes from sustained, non-transactional engagement. Each system gets judged on what it was actually designed to do, and budget flows toward whichever system is underperforming against its own benchmarks rather than against the other system’s metrics.


