Discharge planners, primary care physicians, social workers, elder law attorneys, and adult children of aging parents all send clients to home care agencies. Each gatekeeper works on a different timeline, fears a different bad outcome, and responds to different proof. A single referral partner messaging strategy fails at least four of those five audiences.
TL;DR: Referral source segmentation means mapping each gatekeeper’s primary fear, required proof point, and preferred communication rhythm. A discharge planner who needs a 24-hour intake guarantee and an elder law attorney who needs documented compliance history will never respond to the same brochure. Build separate messaging tracks for each.
Why One Message Fails Five Audiences
Care decision journey mapping starts with a fact that most agencies ignore: referral gatekeepers are solving different problems when they send a client your way. A hospital discharge planner is managing bed turnover and readmission risk. A primary care physician is managing chronic-care continuity. A social worker is managing safety and family dynamics. An elder law attorney is managing liability and Medicaid spend-down timelines. And an adult child is managing guilt, confusion, and urgency.
Research published in the Journal of Aging and Social Policy found that client characteristics directly predict which gatekeeper initiates a referral. Clients with poorer functional ability were more likely to be referred by health workers — physicians, nurses, and discharge planners. Clients with behavioral problems were more likely to enter through non-health-worker channels like family or social services. Female clients and clients cared for by their parents were also statistically less likely to receive health-worker-initiated referrals.
These patterns tell you something important. Your referral sources aren’t interchangeable funnels. They’re separate intake pipelines, each triggered by different client profiles and clinical situations. Multi-audience marketing home care demands that you map these differences before writing a single outreach email or leave-behind.

Hospital Discharge Planners Need Speed Above Everything
Discharge planners work on the tightest timeline in the entire referral ecosystem. Their core fear is a preventable readmission. CMS penalizes hospitals up to 3% of total Medicare reimbursement when 30-day readmission rates exceed risk-adjusted benchmarks. For conditions like heart failure, the national average 30-day readmission rate sits around 21%, according to CMS Hospital Compare data. Discharge planners feel that financial pressure every shift.
Your messaging to this audience should lead with operational speed. Brasstacks, a referral strategy consultancy, recommends building “a clear, written rapid response protocol that guarantees intake within 24 hours of discharge.” That 24-hour benchmark is the proof point discharge planners actually care about. They don’t need to hear about your years of experience. They need to know you’ll answer the phone at 4:30pm on a Friday and have a caregiver in the home by Saturday morning.
The ideal leave-behind for this gatekeeper is a one-page rapid-response card. Include your agency’s intake phone number (answered by a person, not a voicemail tree), your average hours from referral to first caregiver visit (track this — if it’s above 36 hours, fix it before printing the card), and your 30-day readmission rate for patients referred from that specific hospital. If you’re already doing referral source identification work, you’ve got the data. Put it on paper.
How Primary Care Physicians Filter Referrals
Primary care gatekeeping changes how patients enter the home care system at a structural level. A study published in the British Medical Journal confirmed that gatekeeping “is associated with more first contact with a general practitioner or a primary care physician and, consequently, less self-referral.” When a PCP controls the referral pathway, your agency never gets to make its case directly to the family. The physician decides for them.
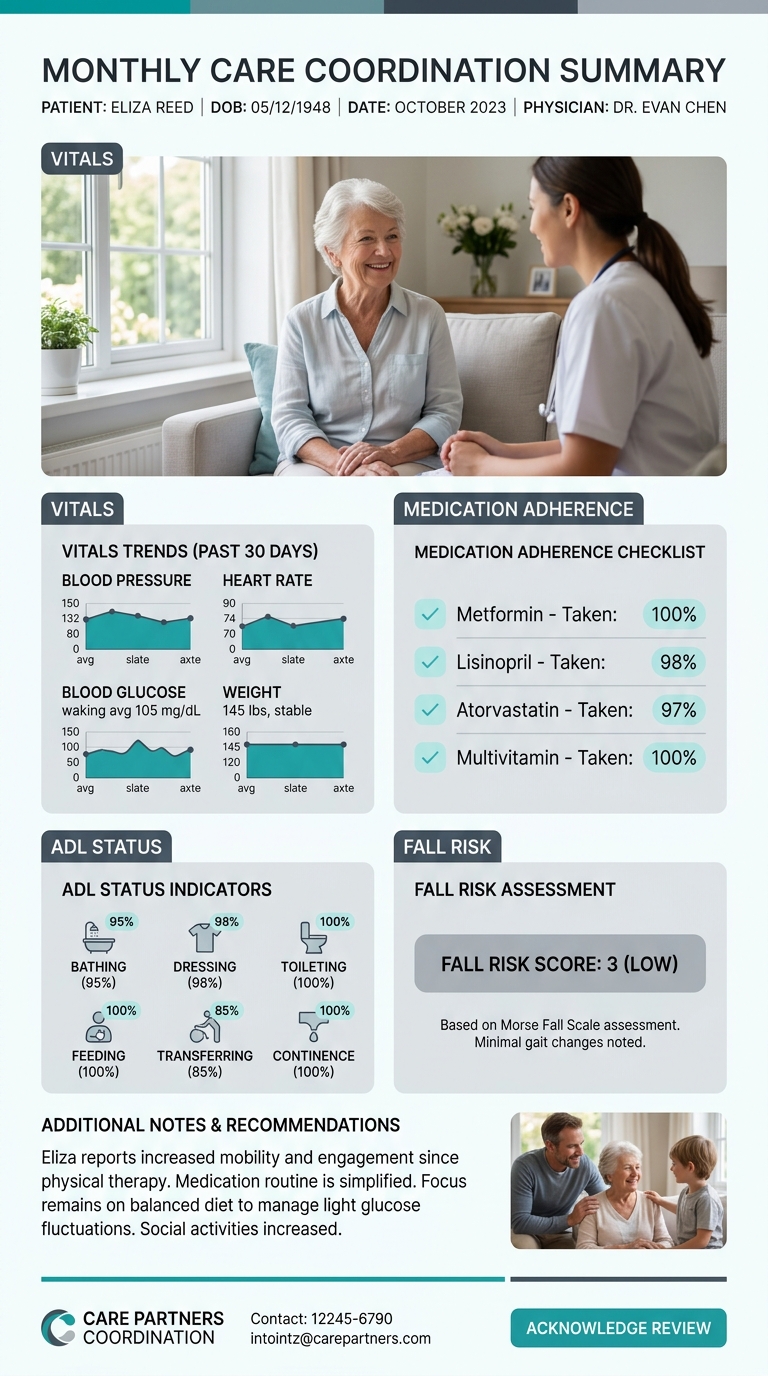
PCPs care about 3 things when choosing a home care partner: clinical reporting quality, medication management support, and communication frequency. Gatekeeper targeting home care through the PCP channel means your messaging should include a sample care coordination report. Show the physician exactly what they’ll receive after each visit: vitals, medication adherence notes, ADL status changes, fall risk scores. If you can commit to sending that report within 48 hours of each home visit, say so explicitly.
Tip: Track your communication compliance rate — what percentage of visits generate a report sent to the referring PCP within 48 hours? If that number is below 90%, fix the process before you pitch the partnership.
A quarterly outcomes summary sent to the referring PCP’s office keeps your agency visible between active cases. Include aggregate numbers: total patients served from that practice, average care duration, hospitalization rate during your services, and client satisfaction scores. PCPs respond to data the way discharge planners respond to speed.
Social Workers and Elder Law Attorneys Weigh Different Factors
Social workers and elder law attorneys both sit in advisory roles, but their decision filters are almost opposite. Social workers evaluate safety, family dynamics, and cultural fit. Elder law attorneys evaluate cost structures, Medicaid compliance, and audit-ready documentation. Grouping them into one “professional referral source” bucket wastes your messaging on the wrong proof points.
For social workers, your outreach should highlight caregiver training credentials, abuse prevention protocols, and multilingual staff availability. Social work referrals in aging services frequently involve family conflict or caregiver burnout. Your agency’s ability to navigate those dynamics — and document that it did so ethically — is the selling point.
For elder law attorneys, the conversation is financial and legal. They want to know your billing is Medicaid-compliant, your documentation can survive an audit, and your contracts have clear scope-of-service language. The DOJ’s 2026 fraud enforcement actions, which charged 455 defendants in schemes totaling $6.5 billion, have made attorneys more careful than ever about which agencies they recommend. Your leave-behind for this audience should include your compliance officer’s direct contact information, a summary of your most recent state survey results, and any accreditation certificates you hold.
Grouping social workers and elder law attorneys into a single “professional referral” category wastes your messaging on the wrong proof points for both audiences.
Health Union’s healthcare audience segmentation research confirms that “segmenting by specialty can help create more targeted campaigns” and that marketers gain insight into pain points only when they collect data from licensing boards and professional associations specific to each group. You wouldn’t send the same email to a geriatric social worker and an estate planning attorney. So stop sending the same brochure.
Family Members Operate on Emotion and Midnight Research
Adult children of aging parents represent the only gatekeeper who is simultaneously the decision-maker, the researcher, and the emotionally overwhelmed party. Research on shared decision-making published in BMJ Evidence-Based Medicine found that effective care decisions require “considering insights that only the patient and perhaps their family can share, insights about both the patient’s biology and biography.” Family gatekeepers carry biographical context that no clinical referral source has.
Their pain points are fear of making the wrong choice, sticker shock, and information overload. Your messaging to families should answer 3 questions within the first 30 seconds of contact: What will this cost per week? Who will be in my parent’s home? What happens if something goes wrong? If your website can’t answer those questions at 11pm — when most family research happens — you’re losing this audience to competitors whose sites can. We’ve explored why after-hours website experience matters for decision-makers in depth.
SageCare’s referral marketing research notes that partners “want reliability, responsiveness, and partners who make their jobs easier,” adding that “your outreach should demonstrate that you understand their goals and can deliver the kind of client experience that reflects well on them.” For family gatekeepers, “making their job easier” means shrinking the cognitive load of a decision they never planned to face. A transparent pricing page, caregiver bios with photos, and a live-answered phone line do this better than any glossy brochure.
Building the Gatekeeper Pain-Point Matrix
The mechanism behind effective referral source segmentation is a framework worth naming: the Gatekeeper Pain-Point Matrix. For each referral source type, you document 3 elements: the gatekeeper’s primary fear (what bad outcome are they trying to avoid?), their required proof point (what evidence resolves that fear?), and their preferred communication cadence (how often and through what channel do they want updates?).
| Gatekeeper | Primary Fear | Required Proof | Communication Cadence |
|---|---|---|---|
| Discharge Planner | Readmission penalties, bed bottlenecks | 24-hour intake guarantee, readmission data | Weekly calls during active referrals |
| Primary Care Physician | Lost care continuity, liability | Post-visit clinical reports, quarterly outcomes | Reports within 48 hours, quarterly summaries |
| Social Worker | Client safety, family conflict | Caregiver training records, abuse prevention protocols | Monthly relationship touchpoints |
| Elder Law Attorney | Fraud exposure, audit failure | Compliance documentation, accreditation certificates | Quarterly regulatory updates |
| Family Member | Wrong-choice guilt, financial surprise | Transparent pricing, caregiver bios, emergency plan | Immediate intake response, weekly care updates |
ReferralRock’s home care research reinforces that agencies should “include specific details that highlight your unique connection with the referrer” in every touchpoint. The matrix gives you those specific details by gatekeeper type. When Care Marketing’s team works with agencies on referral partner messaging strategy, this matrix is the starting document — before any copy gets written.
Where the Map Breaks Down
The Gatekeeper Pain-Point Matrix works cleanly when each referral source fits one category. Real life is messier. A social worker at a hospital functions partly as a discharge planner. A PCP in a concierge practice gives advice that resembles an elder law attorney’s counsel. A family member who is also a registered nurse brings clinical expectations that don’t match the standard family-gatekeeper track.
The matrix also assumes your agency can deliver on every proof point it promises. If your real average intake time is 52 hours but your rapid-response card says 24, a discharge planner will refer to you exactly once. If your post-visit reports go out 5 days late, the PCP relationship erodes within a quarter. ContentMation’s 2026 healthcare referral marketing analysis warns that agencies must ensure “every campaign meets HIPAA, FDA, and FTC guidelines” — and that operational reality has to match marketing promises, because compliance-focused referral partners will verify your claims.
The biggest limitation of care decision journey mapping is that it can’t account for relationship depth. An agency with a 10-year personal bond to a discharge planner will get referrals despite having a slower intake process. An agency with a perfect matrix but zero in-person history will lose to the competitor whose rep brings coffee every Thursday morning. The map gives you the right message for each gatekeeper. But if your referral relationships develop gaps after the first meeting, no document can close them. Delivery still depends on a real person who shows up, follows through, and treats every promise as a contract.


