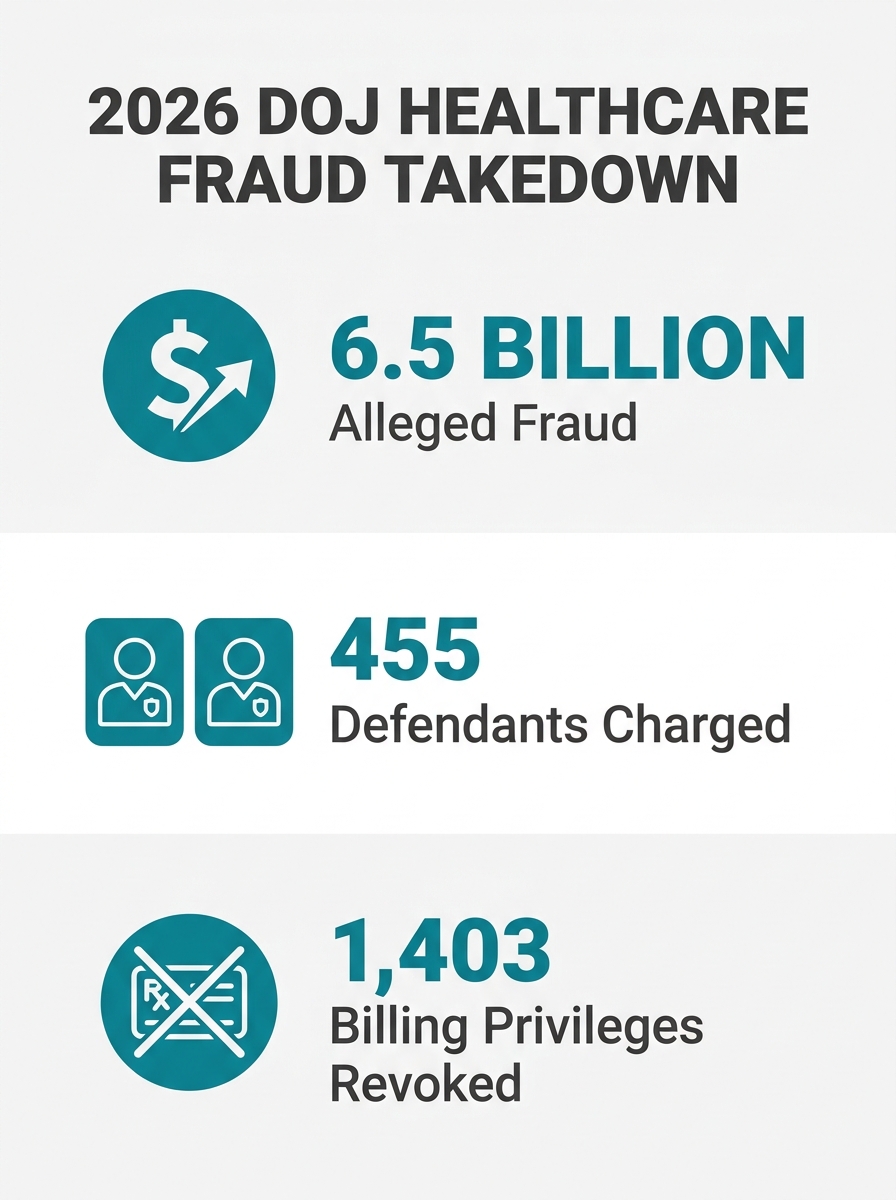
The Department of Justice charged 455 defendants on June 24, 2026, in alleged healthcare fraud schemes totaling $6.5 billion. Home health and personal care agencies are explicitly named as high-risk service lines, and this enforcement action signals a permanent shift in how federal investigators scrutinize billing, documentation, and marketing claims accuracy.
56 Federal Districts, One Coordinated Sweep
The 2026 National Health Care Fraud Takedown, the first operation executed under the DOJ’s newly created National Fraud Enforcement Division (NFED), spanned 56 federal districts across 45 states and territories. Of the 455 defendants charged, 295 face allegations tied to Medicaid fraud involving more than $518 million in false claims. All 50 state Medicaid Fraud Control Units participated simultaneously for the first time in enforcement history.
CMS suspended 1,079 providers and revoked billing privileges for another 1,403 during the operation. HHS-OIG excluded more than 1,400 providers from federal healthcare programs and is pursuing over $10 billion in potential recoveries. The government seized $182 million in physical assets, including cash, luxury vehicles, and jewelry, and secured $73 million across 48 Civil Monetary Payment settlements.
The fraud patterns documented in the charges follow familiar categories: billing for services never rendered, billing for medically unnecessary services, kickback schemes, and falsified documentation. Ninety of the 455 defendants are doctors or licensed medical professionals. The National Law Review’s analysis of the takedown put it bluntly: “Medicaid risk should be treated as an enterprise-level compliance priority, particularly in high-risk service lines such as behavioral health, personal care, home health, and adult day care services.”
If you run a home care agency that bills Medicaid, the message here is concrete: healthcare fraud prevention 2026 priorities place your service line in the enforcement spotlight alongside behavioral health and adult day care. This isn’t a peripheral risk category. It’s the one prosecutors chose to build their largest-ever coordinated operation around.
How the Government Finds Billing Anomalies Before Whistleblowers Do
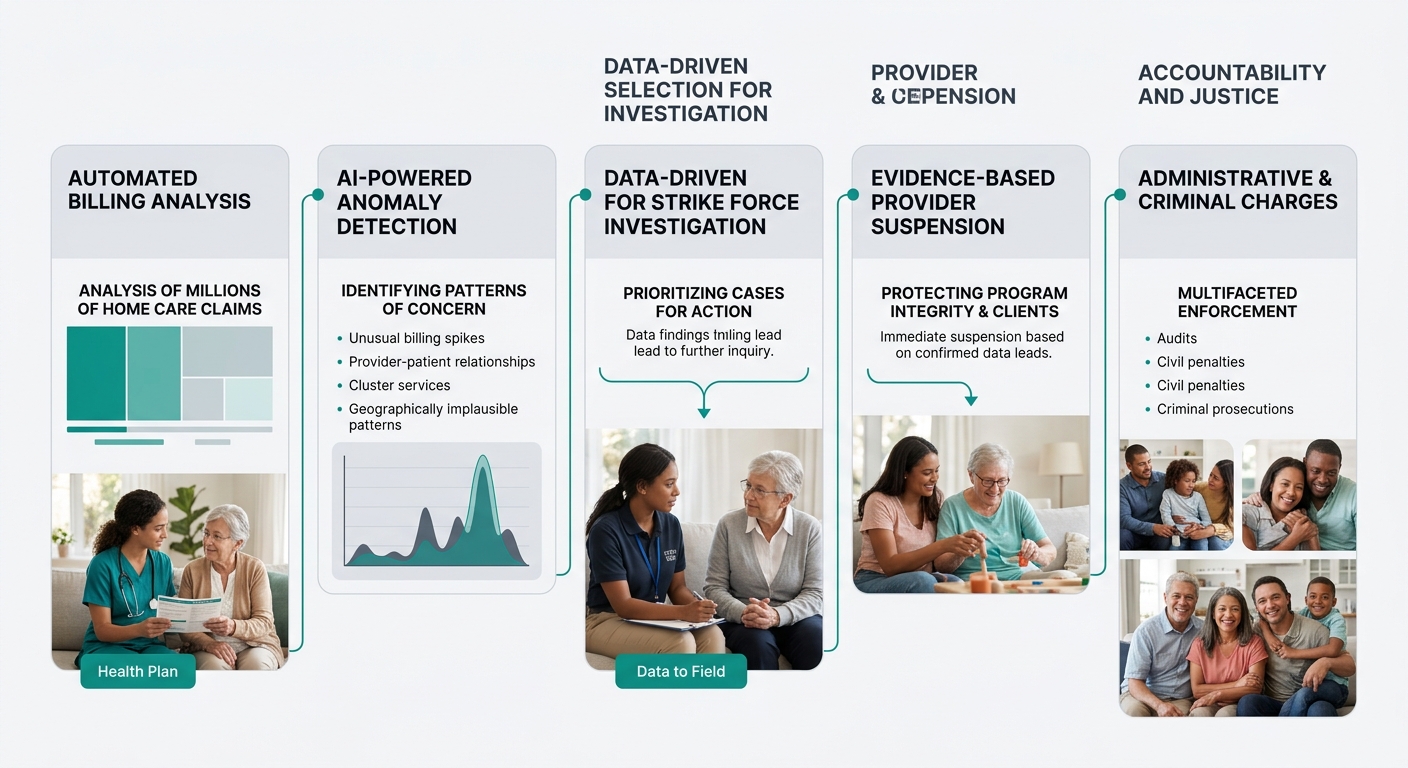
The enforcement methodology behind this takedown differs from prior years. The DOJ and CMS are now using AI-powered data analytics and pattern-matching algorithms to flag billing outliers before a qui tam relator or whistleblower ever picks up the phone. The NFED was built specifically to centralize these capabilities and deploy them through regional Strike Forces covering the West Coast, Midwest, and other territories.
What does this mean for a 40-caregiver home care agency in suburban Ohio? It means the same algorithmic scrutiny that caught multi-million-dollar fraud rings is scanning your claims data too. If your billing patterns deviate from local or regional norms, the flag goes up automatically. No disgruntled employee has to file a complaint. No competitor has to report you. The system finds anomalies on its own.
Bill Essayli, head of the Central District of California’s U.S. Attorney’s office, described the current enforcement posture with a phrase that should keep compliance officers awake: “This is the beginning.” The Pillsbury Law analysis of his remarks warned that “this uptick in government enforcement is sure to spur qui tam relators and whistleblowers” and that “unprepared California hospice and home health companies may face significant civil, and even criminal, exposure.”
The data-driven approach creates a specific compliance demand around Medicaid documentation transparency. Every visit note, every EVV timestamp, every plan-of-care update becomes a data point that either supports your billing or contradicts it. CMS requires certified home health agencies to maintain documentation covering medical necessity, OASIS assessments, and detailed plans of care. Service notes, EVV data, and MCO-specific requirements must align with every claim submitted, with timely filing deadlines typically running 90 to 365 days after the date of service.
Warning: If your documentation workflow relies on caregivers completing visit notes hours or days after the actual visit, you’re generating exactly the kind of data inconsistency that pattern-matching algorithms are trained to detect. Real-time or same-day documentation closes this gap.
When Your Marketing Copy Becomes Evidence
Here’s where the takedown intersects with something most home care marketers don’t think about: the claims you make on your website, in your brochures, and during family consultations can become evidence in a fraud investigation. If your marketing promises services or outcomes that your documentation can’t support, you’ve created a paper trail that prosecutors know how to read.
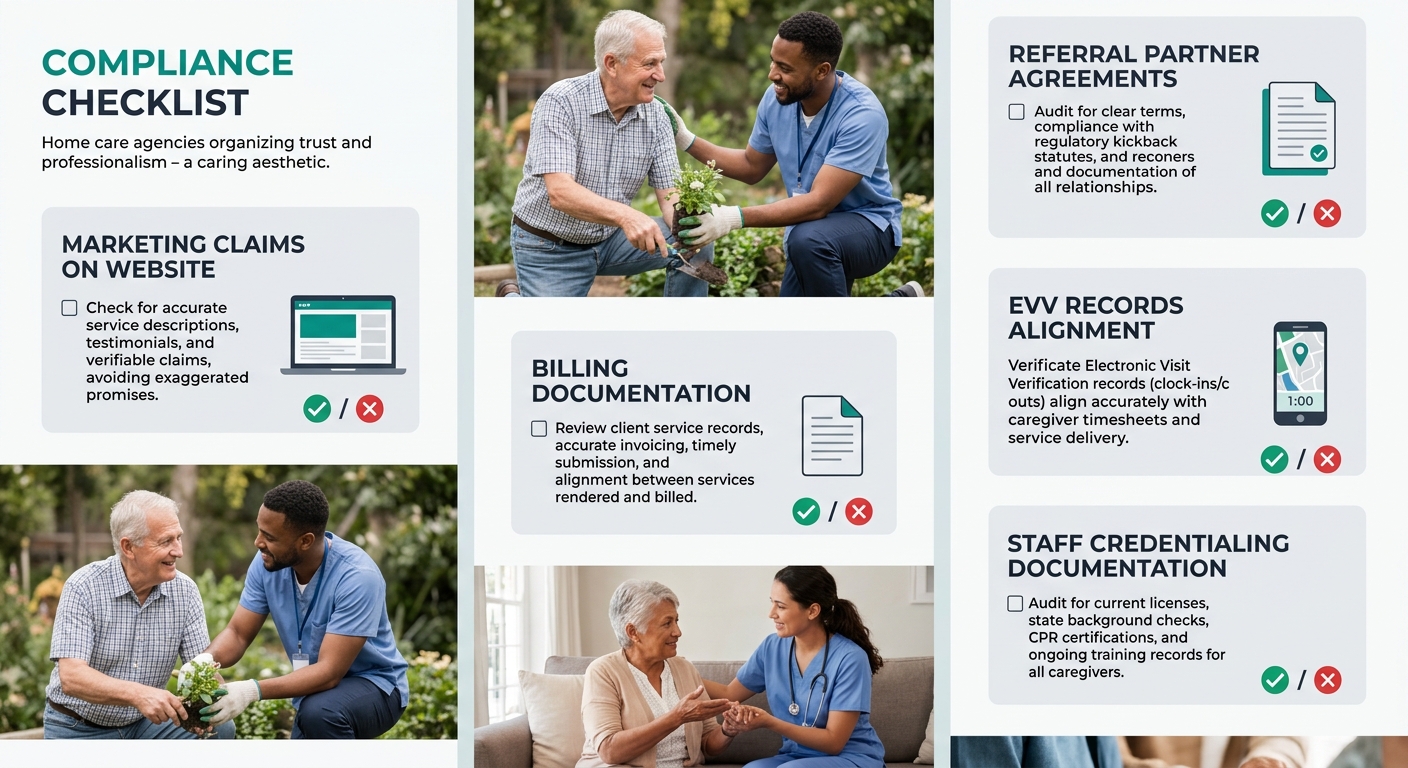
Home care compliance marketing requires that every clinical claim on your website is substantiated, every statistic you cite is sourced, and every outcome representation includes appropriate context. The FTC enforces truth-in-advertising standards that apply to health claims, and HIPAA governs how patient data can appear in marketing materials. As one compliance guide notes, “informed consent doesn’t start in the exam room; it starts in your marketing.”
Consider a practical example. Your website says “our clients show a 40% reduction in hospital readmissions.” If you can’t produce the data behind that number tied to your actual client population, that claim is a compliance liability. It’s also an FTC violation. And if an investigator looking at your Medicaid billing finds that your documented outcomes don’t match your marketing language, you’ve handed them a narrative about an agency willing to misrepresent results.
If an investigator looking at your Medicaid billing finds that your documented outcomes don’t match your marketing language, you’ve handed them a narrative about an agency willing to misrepresent results.
The same logic applies to how you describe your staff qualifications, your service availability, and your specializations. We’ve written before about why vague care language costs you more than you think, and the compliance dimension adds real legal weight to that argument. Marketing claims accuracy requires a direct line between what your website says and what your internal records show.
Agencies running paid campaigns through Google or Facebook should audit their ad copy with the same rigor. Claims like “24/7 care available” or “specialized dementia support” need to be backed by staffing records and training documentation. If you’re advertising capabilities you can’t consistently deliver, you’re building a compliance problem one click at a time.
Referral Relationships Under the Anti-Kickback Statute
The 2026 takedown also charged defendants with kickback schemes, which carries specific implications for how home care agencies build and maintain their referral networks. The Anti-Kickback Statute makes it a federal crime to offer, pay, solicit, or receive anything of value to induce referrals for services covered by federal healthcare programs.
Referral partner vetting has to go beyond asking whether a hospital discharge planner or physician office sends you good leads. You need to understand whether your referral arrangements could be characterized as inducements. Paying referral fees to individuals, offering gift cards to case managers, or providing free services to facilities that send you patients all fall within the statute’s scope.
Building referral relationships the right way means focusing on clinical quality and communication, as referral source strategies for home care should center on demonstrable outcomes and documented competency rather than financial incentives. Doctors and facilities want to partner with agencies that employ skilled clinicians who communicate clearly and uphold high standards, according to Alora Health’s analysis of referral relationship building. When you vet your own referral partners, the same scrutiny applies in both directions. Partnering with facilities or providers that have compliance problems of their own can drag your agency into investigations you had nothing to do with. The assisted living referral relationship model works the same way: make sure the partners you’re sending families to maintain standards as high as yours.
If your agency is ever pulled into a fraud investigation, the quality of your crisis communication planning will determine whether you survive the reputational damage. Having a documented response protocol isn’t paranoia. Given the scale of the 2026 takedown, it’s operational hygiene.
The Enforcement Pipeline After June 2026
Bill Essayli’s “this is the beginning” statement isn’t rhetorical positioning. The structural changes behind this takedown, including the creation of NFED, the deployment of AI-driven billing analysis across all 50 states, and the coordination of every state Medicaid Fraud Control Unit, represent permanent infrastructure. These capabilities don’t get dismantled after a press conference. They get refined.
For home care agencies, the practical response breaks down into three areas that need attention before the next enforcement cycle.
Documentation discipline. Every visit note, care plan update, and service record must match your billing submissions exactly. CMS, HIPAA, and Medicare documentation standards apply to all certified agencies regardless of state. Timely filing, denial tracking, and OASIS compliance aren’t administrative tasks you can delegate without oversight. They’re the data that either protects you or exposes you.
Marketing audit. Walk through every page of your website, every brochure, and every ad campaign with a compliance lens. Can you substantiate every clinical claim? Can you source every statistic? Do your outcome representations include appropriate context? If not, fix them before someone else reads them with subpoena power.
Referral structure review. Document every referral relationship your agency maintains. Confirm that no arrangement could be characterized as an inducement under the Anti-Kickback Statute. If you’re uncertain about any partnership’s structure, get a healthcare attorney’s opinion in writing.
The 2026 takedown charged 455 people and disrupted billions in alleged fraud. The enforcement apparatus that produced those results is still running, still learning from the data it collects, and still building cases. Agencies that treat home care compliance marketing and Medicaid documentation transparency as operational priorities, rather than annual checkbox exercises, are the ones that will still be operating when the next round of charges drops.


