The testimonial page on your home care website converts families at a reasonable clip and does absolutely nothing for the hospital discharge planner deciding where to send twelve patients this quarter. Your client success stories are written for the wrong audience, structured around the wrong proof points, and published in channels your referral partners never check.
TL;DR: Referral partners — discharge planners, physicians, social workers — need clinical outcomes, operational reliability metrics, and rapid-response proof. Family-facing testimonials built around emotional gratitude don’t answer those questions. Repurposing testimonials for healthcare referral audiences requires rewriting them from scratch around a different evidence set, then distributing through partner-specific channels.
Discharge Planners Need Data, Not Gratitude
Why do referral partner testimonials fail when they come straight from your family-facing library? Because a discharge planner’s decision criteria share almost nothing with a family’s. Families ask “Will my mom be safe and happy?” Discharge planners ask “Will this agency pick up the phone at 4pm on a Friday, staff the case within 18 hours, and send me documentation I don’t have to chase?”
The disconnect runs deep. As OneIMS’s guide on B2B testimonials puts it, “A customer testimonial or case study should not be about you or your B2B organization — it should be about the customer.” In referral partner terms, the customer is the discharge planner or physician, not the family. The testimonial needs to solve their problem, and their problem is operational risk.
Look at what a typical home care client story includes: a family member describing how a caregiver became part of the household, a mention of reliability, a vague reference to “peace of mind.” Now look at what a discharge planner at a 300-bed hospital actually tracks before choosing a home care partner: time-to-staff (measured in hours), missed-visit rates (measured as a percentage), 30-day rehospitalization rates for patients referred to your care, and communication responsiveness measured by callback windows.
A testimonial that says “They were wonderful with Mom” gives a discharge planner zero usable information. A testimonial from a fellow discharge planner that says “They staffed 94% of referrals within 18 hours and our 30-day readmission rate dropped from 14% to 9% for patients they handled” answers every question that matters. One of those two versions builds a referral relationship. The other gets filed in the same mental category as the branded pen your liaison left on the counter.
The Client Success Story Structure That Actually Moves Physicians
The American Medical Association’s guide to physician referral strategies is direct: content marketing establishes thought leadership, SEO enhances visibility, and maintaining a positive online reputation is crucial for building trust and referrals among peers. Physician referral content has to do real clinical work. A story about a satisfied daughter doesn’t meet that bar.
Be More Effective’s guidance on testimonial collection reinforces this point: the conversation preceding a testimonial request works best when it focuses on the value you’ve delivered by solving a problem, digging them out of a hole, or delivering something above specification. You need to identify the specific problem you solved for the referral partner, not the family.
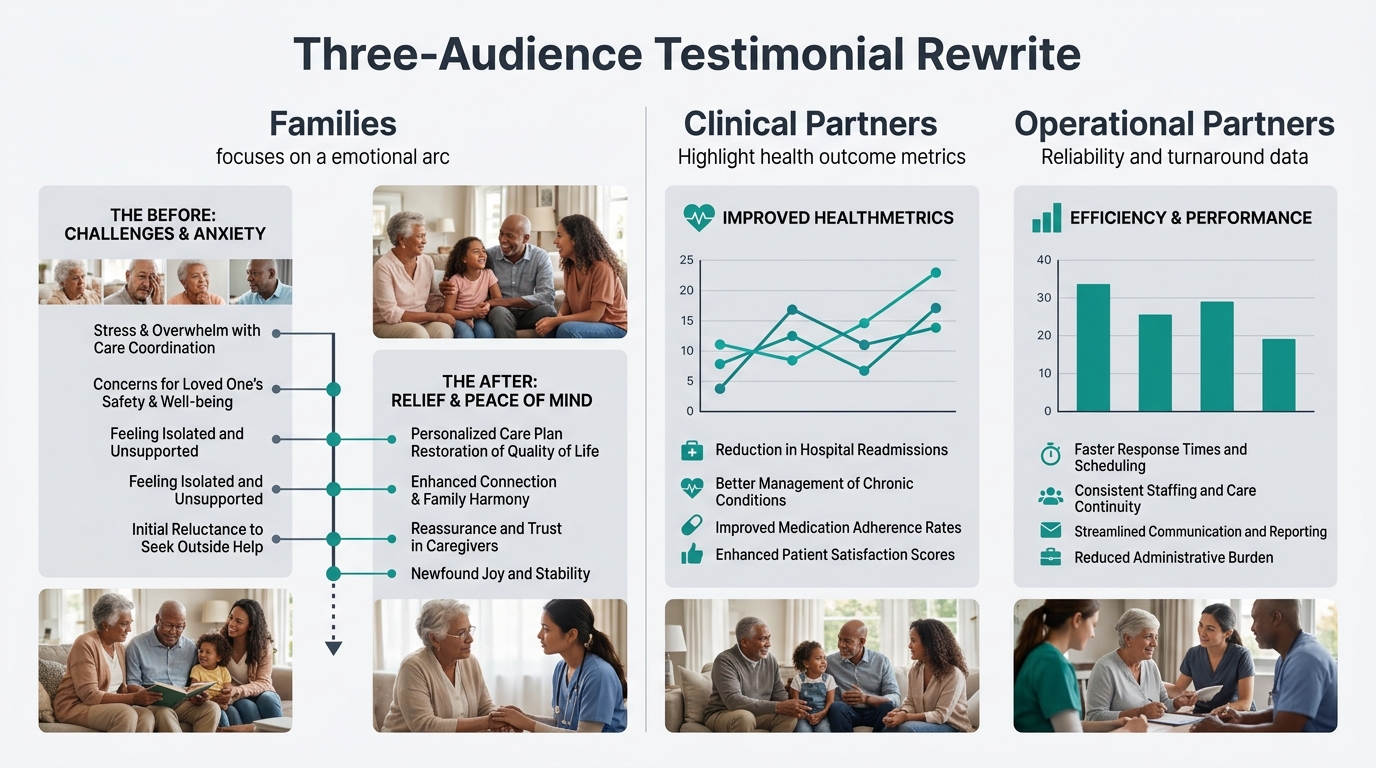
Here’s the client success story structure that converts referral partners. I call it the Three-Audience Testimonial Rewrite:
Audience 1: Families. Emotional arc. Challenge → caregiver match → quality of life improvement. This is what you already have, and it works fine for its intended purpose.
Audience 2: Clinical referral partners (physicians, nurse practitioners). Clinical arc. Diagnosis or condition → care plan coordination → measurable health outcome. Include fall reduction percentages, medication adherence rates, ER visit frequency changes. Quote the referring clinician, not the family.
Audience 3: Operational referral partners (discharge planners, social workers, case managers). Operational arc. Referral speed → staffing reliability → documentation turnaround → ongoing communication frequency. Quote the partner about how working with your agency reduced their administrative burden.
Every strong client story in your library contains the raw material for all three versions. The family story is version one. Versions two and three require you to go back to the clinical and operational contacts involved in that same case and collect different data points from different people.
This is where the concept of testimonial repurposing for healthcare referral audiences gets practical. You’re not slapping a different headline on the same content. You’re extracting three separate narratives from one care episode, each with its own protagonist, its own success metric, and its own distribution channel.
Every strong client story in your library contains the raw material for three versions. The family story is version one. Versions two and three require going back to the clinical and operational contacts and collecting entirely different data from entirely different people.
You’re Publishing Where Partners Never Look
Conversion rate optimization research consistently shows that placement determines impact. Optimized page placement drove a 43% revenue increase in one documented case study and a 12% lift in orders in another, and A/B testing on placement achieved a 56% success rate across Convertcart’s portfolio of experiments. Testimonial placement works the same way for your agency. Position matters as much as content.
Where do you currently publish client stories? Your website’s testimonial page. Your Google Business Profile. Maybe your Facebook page. Your printed brochure.
Where do your referral partners actually evaluate you? Inside their EHR’s preferred-provider directory. In the PDF one-pagers your liaison drops off at the nurses’ station. In the follow-up email after a lunch-and-learn. In your referral partner portal, if you’ve built one.
The gap between those two lists explains the conversion failure. The family who left a glowing 5-star Google review is visible to other families searching “home care near me.” That same review is invisible to the discharge planner who uses an internal referral list she hasn’t updated since she attended your open house 14 months ago.
Referral partner testimonials need to travel through referral partner channels:
- One-pagers for liaison visits featuring a quote from a peer at a comparable facility, with 2-3 outcome metrics bolded at the top
- Email sequences triggered after a referral partner sends their first case to you, including a 60-second video testimonial from another partner. Research from Testimonial Hero confirms that video testimonials with a clear call to action outperform text-only formats for B2B audiences.
- Quarterly outcome reports that function as recurring testimonials by showing aggregate data: average time-to-staff across all referrals, missed-visit rate, partner satisfaction scores from your last survey
If you’re already producing video content, the in-house vs. outsourced production decision matters here. A 60-second partner testimonial shot on an iPhone in a hospital conference room carries more credibility than a polished studio piece, because it looks like what it is: a real professional vouching for you between meetings.
Tip: When collecting referral partner testimonials, ask partners about the channels they prefer, the timing of your requests, and any perceived barriers in the referral relationship. Use that feedback to refine both the testimonial content and your referral process. The collection conversation doubles as a relationship-building opportunity.
And none of this matters if your broader reputation management for home care falls short. A discharge planner who hears a strong testimonial from a peer and then Googles your agency to find a 3.2-star rating with unaddressed complaints will discard the testimonial entirely. The partner testimonial opens the door. Your online reputation has to hold up when they peek through it.

Where This Leaves Your Testimonial Library
The thesis holds up, and it holds up uncomfortably. The glowing family stories you’ve spent years collecting serve a real purpose for family-facing marketing, but they are functionally irrelevant to the referral partners who drive your highest-converting, highest-lifetime-value client channel.
The fix requires three separate workstreams. You need to audit existing client stories for cases where you can go back and collect clinical and operational data from the professionals involved in that care episode. You need a distinct collection process for referral partner testimonials that asks different questions, targets different respondents, and captures metrics like staffing speed and readmission rates instead of emotional satisfaction. And you need distribution infrastructure that puts partner-facing proof in partner-facing channels instead of burying it on a webpage designed for anxious adult children searching at 11pm.
A mix-and-match approach across audiences and formats tends to produce the strongest results for testimonial programs overall. The agencies that build all three versions of the Three-Audience Testimonial Rewrite will have a referral conversion advantage that compounds quarter over quarter, because every new partner testimonial makes the next liaison visit more productive and the next referral conversation shorter. The agencies that keep sending family stories to discharge planners will keep wondering why the lunch-and-learn went well but the referral numbers never moved.


