Referred clients convert at a 30% higher rate, retain 37% better, and carry 16% more lifetime value than non-referred clients, according to CareSmartz360 tracking data. But those aggregate numbers hide a critical distinction: the source of the referral matters more than the referral itself, and your happiest families are rarely your highest-yield growth channel.
TL;DR: Client advocates generate warm leads, but professional referral partners (discharge planners, social workers, skilled home health providers) produce higher-volume, better-matched referrals that convert more reliably. Segmenting referral sources into tiers and measuring conversion rate by source, instead of as a blended average, changes where you invest your relationship-building time.
Thirty Percent of Referrals Fail Before They Start
A significant share of home care referrals never convert because the client’s needs don’t match the agency’s services. An AutomationEdge study found that 30% of referrals in home healthcare are rejected due to service-offering mismatches. The referral came from someone who didn’t fully understand what the agency could deliver. This rejection rate hits client-advocate referrals disproportionately. A grateful daughter who refers her neighbor to your agency doesn’t know whether you handle dementia care, medication management, or overnight shifts. She knows you were good to her mother.
That emotional endorsement carries real weight. Personal endorsements are up to 50 times more effective than standard advertising, according to ReferralRock’s analysis of consumer research. But weight and precision are different things.
Professional referral sources, such as hospital discharge planners, geriatric care managers, and skilled home health nurses, refer with clinical specificity. They know your license type, your geographic coverage, your staffing capacity for specialized cases. Their referrals arrive pre-qualified in ways a family advocate’s referrals almost never do.
Client Advocates Rank High on Loyalty, Low on Scalability
Satisfied families are essential to your reputation. They leave Google reviews, they tell their church group, they reassure anxious friends. Their value to your agency is real. But measuring client referral conversion rates in isolation creates a misleading picture of growth potential.
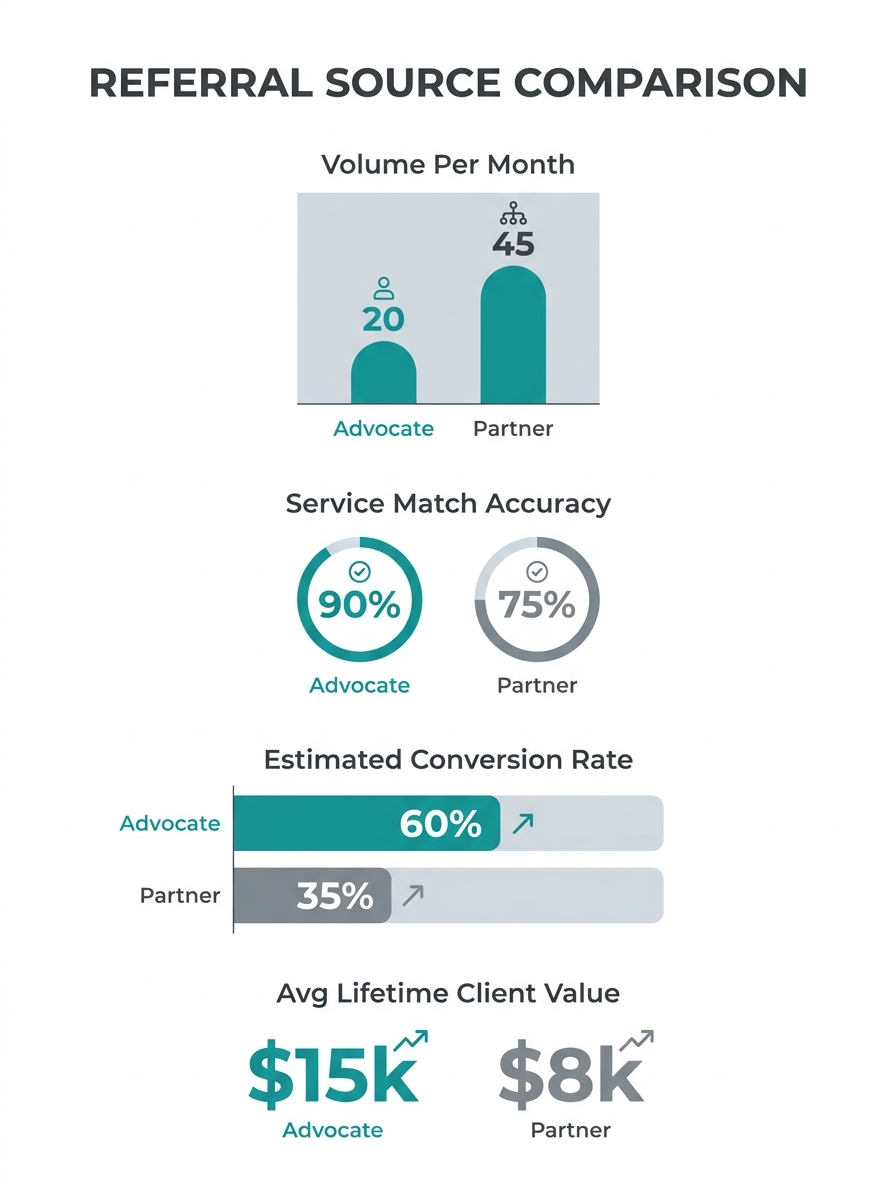
Here’s the math that trips agencies up. A typical home care agency might have 80 to 120 active clients at any given time. Even highly satisfied clients generate referrals at low, sporadic rates, often producing 2 to 5 family-sourced referrals per month from a client base of 100. A single active discharge planner at a mid-sized hospital, by contrast, can generate 3 to 8 qualified referrals per week.
The volume gap compounds over quarters. And when you factor in the 30% service-mismatch rejection rate that skews toward client-sourced referrals, the effective yield difference widens further.
One Forbes Agency Council contributor described the dynamic in an April 2025 piece: “Our biggest referral partners are consultants offering complementary services… They bring us clients who need more leads, and we help their clients generate higher-quality leads, creating a win-win cycle of success.” The principle applies directly to home care: your growth engine is the professional who needs you to complete their own care continuum, not the family member who loves you.
Professional Partners Convert on a Different Curve
Referral programs, when properly tracked and optimized, deliver 30x average ROI, according to Rivo’s analysis of program performance data. Harvard Business Review research cited in the same analysis found that referred customers generate higher margins and stronger long-term retention. But that 30x figure reflects structured programs with defined partner relationships, not organic word-of-mouth from happy clients.
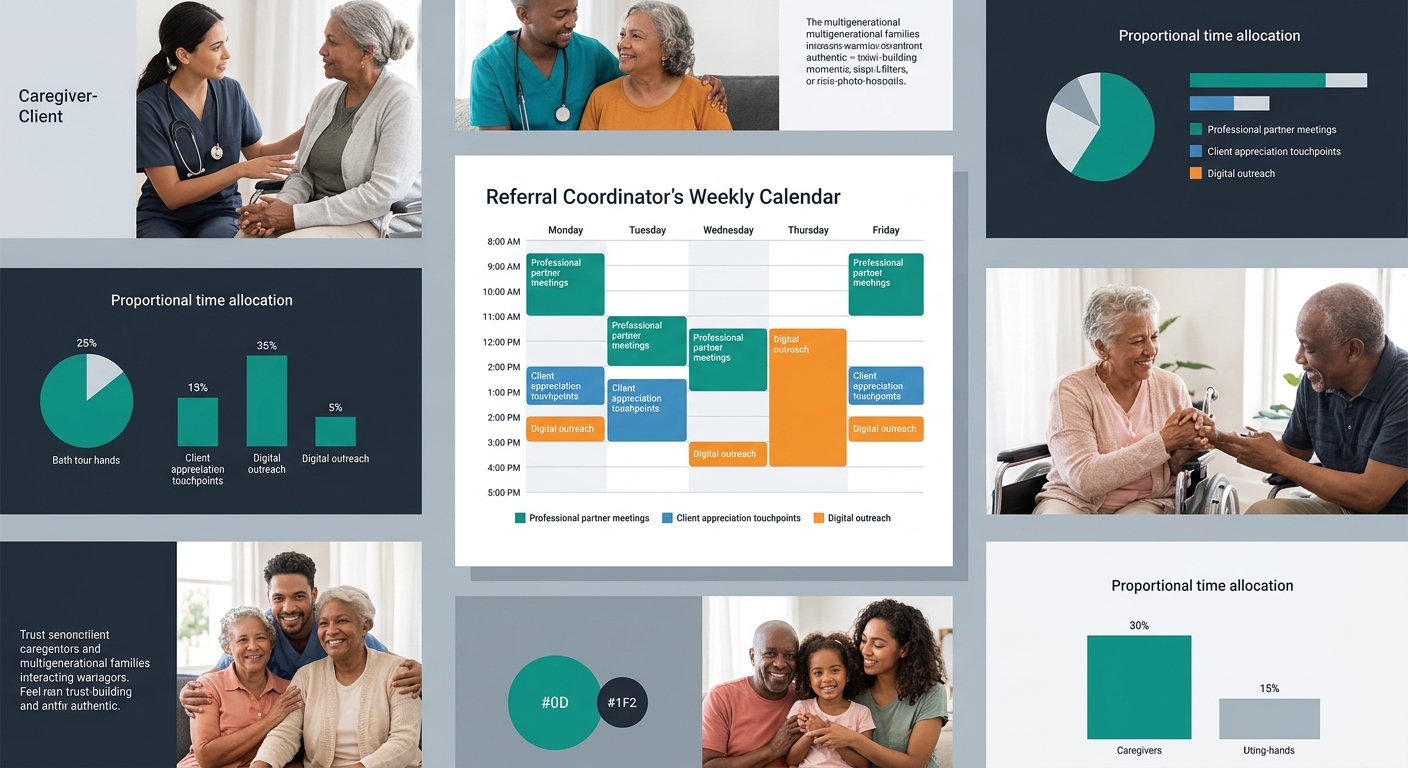
The distinction matters for how you allocate your referral coordinator’s time. If your coordinator spends 60% of their week maintaining relationships with 5 to 8 key professional partners (discharge planners, elder law attorneys, skilled home health agencies, geriatric care managers), they’re working the high-conversion channel. If they spend the same proportion running client appreciation events and hoping for organic mentions, they’re working a channel with real but limited throughput.
GetTheReferral’s contractor ROI guide frames the accountability standard bluntly: “If your referral program brought in $200,000 in revenue and cost $20,000 to run, your ROI is 10X. The real power comes from breaking this down further.” That breakdown, by source, by tier, by quarter, is exactly where most home care agencies stop short. They track total referrals, total conversions, total revenue. They don’t track which source types drive the 10X and which drag it down to 3X.
Brasstacks, a home care consulting firm, reinforces the professional-partner advantage in their referral strategy guide: collaborations between skilled home health providers and non-medical care agencies are “mutually beneficial” because “jointly tracking outcomes can demonstrate how your combined services reduce hospitalization.” That outcome-tracking creates a feedback loop. The professional partner sees data proving your agency improves their patients’ results, which increases their referral confidence and frequency. No client advocate generates that kind of data-backed referral acceleration.
Your happiest family isn’t your best referral source. Your most active discharge planner is.
The Three-Tier Referral Segmentation Model
Effective referral partner prioritization requires sorting your sources into tiers based on volume, match quality, and conversion rate. Advanced referral strategies in adjacent industries already use tiered segmentation, placing high-value professional partners in Tier 1 and community-level advocates in Tier 2. Home care agencies benefit from a three-tier version.
| Tier | Source Type | Examples | Typical Monthly Volume | Est. Conversion Rate | Contact Frequency |
|---|---|---|---|---|---|
| 1 | Institutional clinical | Hospital discharge planners, SNF social workers, home health agencies | 12–32 per partner | 45–60% | Weekly |
| 2 | Professional non-clinical | Elder law attorneys, geriatric care managers, financial advisors, faith leaders | 3–8 per partner | 30–45% | Biweekly |
| 3 | Client advocates | Satisfied families, current clients, former clients | 2–5 total | 20–35% | Quarterly nurture |
The conversion estimates draw from benchmarks in CareSmartz360 and LeadSquared tracking guidance. Your actual rates will vary by market, payer mix, and service scope. The point is to track home care agency growth metrics at the tier level, not as a single blended referral number.
If you’ve built a referral partner portal or CRM structure to manage these relationships, tagging each source by tier gives your referral coordinator a clear weekly priority list. And if you’ve made common first-meeting errors with professional partners, the tier framework helps you identify which recovery efforts deserve urgent attention (Tier 1) versus which can wait (Tier 3).
The Generational Shift Complicating Referral Strategy
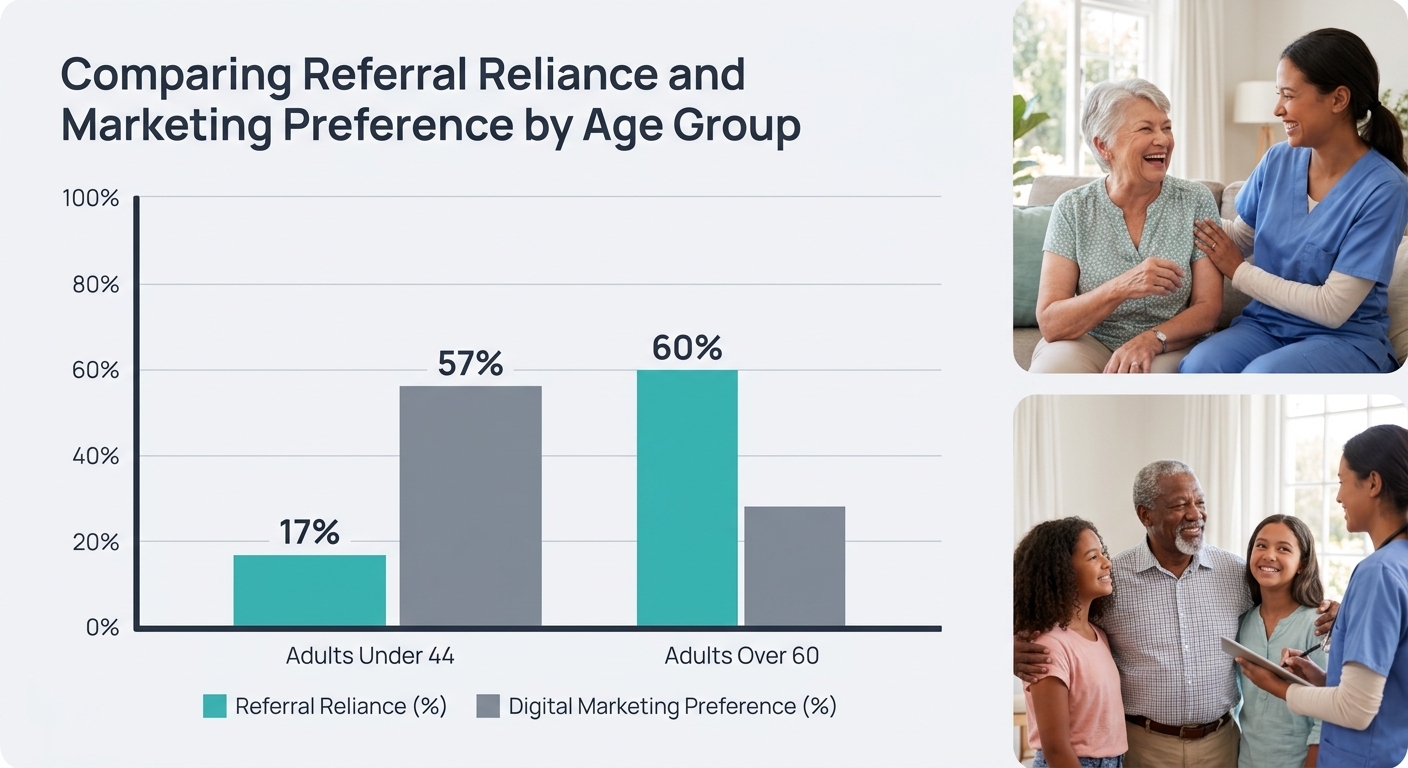
Referral source segmentation gets harder when you factor in how younger family decision-makers find care. Industry data from 2025 shows that 76% of advisors in adjacent care fields gained new clients through unsolicited referrals, but only 17% of decision-makers under 44 require a referral before engaging a provider. Meanwhile, 57% of younger buyers select providers through digital channels, compared to 60% of those over 60 who still rely on referrals.
For home care agencies, this means the adult children making care decisions for aging parents are increasingly bypassing the referral channel entirely. They search Google. They read reviews. They compare pricing pages. They visit your website at 11pm on a Tuesday and expect to find answers without calling anyone.
This doesn’t eliminate the value of professional referral partners. Discharge planners will keep referring regardless of the family’s age because the referral happens within a clinical workflow, not a consumer search. But it does mean that your Tier 3 (client advocate) channel will erode faster than your Tier 1 channel over the coming years. Investing in content marketing for care providers and email marketing for care providers fills the gap that shrinking organic word-of-mouth leaves behind.
What Tier-Level Data Leaves Unresolved
The three-tier model gives you a prioritization framework, but several questions remain open. The 30% service-mismatch rejection rate, for instance, comes from aggregate home healthcare data. No published study breaks that figure down by referral source type. We’ve argued that client advocates contribute disproportionately to mismatches based on their lack of clinical knowledge, but confirming that requires your own tracking.
Similarly, the 30x ROI figure for referral programs reflects structured B2C and B2B programs across industries, not home care specifically. Home care operates under Stark Law and Anti-Kickback Statute constraints that limit how you can incentivize professional referrals, making direct ROI comparison difficult. LeadSquared’s referral source guide emphasizes consulting legal experts to align referral approaches with local and national regulations, and that compliance layer changes the cost structure of partner programs in ways generic ROI benchmarks don’t capture.
The generational data (17% of under-44 decision-makers needing referrals, 57% choosing through digital channels) comes from financial advisory research, not home care directly. The directional trend almost certainly holds across service categories, but home care-specific generational conversion data remains sparse. If you’re tracking referral source segmentation in your CRM and tagging by tier, by quarter, and by payer source, you’re building a local dataset that will tell you more about where your next 50 clients will come from than any national benchmark can.


