Thirty percent of consumers follow brand recommendations when choosing a service provider, according to Nielsen Commspoint Journey data cited in a homecare referral guide from A Place at Home. In home care, where a daughter is deciding who will help her aging mother get out of bed each morning, that figure almost certainly understates the influence of referrals. Yet open a typical agency’s KPI dashboard and the referral picture is either missing entirely or reduced to a single hand-typed column at intake: “hospital,” “Google,” “friend,” blank. The rest of the screen glows with click-through rates, cost-per-lead figures, and website sessions that tell you plenty about your ad spend and almost nothing about why families actually picked up the phone.
This gap between what your dashboard measures and what drives client acquisition is where agencies lose both budget and strategic clarity. The problem isn’t that your KPIs are wrong. They measure real things. But they measure the things that are easiest to count, and referral relationships have never been easy to count.
The Dashboard You Built Tracks Transactions, Not Relationships
Think about how your current home care agency KPI tracking actually works. Your Google Ads account reports impressions, clicks, and form fills. Your website analytics show session duration and page views. If you’re running home care paid ads through a managed campaign, you can see cost-per-acquisition down to the keyword level. These are transactional metrics, and they’re useful for optimizing individual channels. Where they fail is in representing the full path a family takes before becoming a client, which rarely begins and ends inside a single channel.
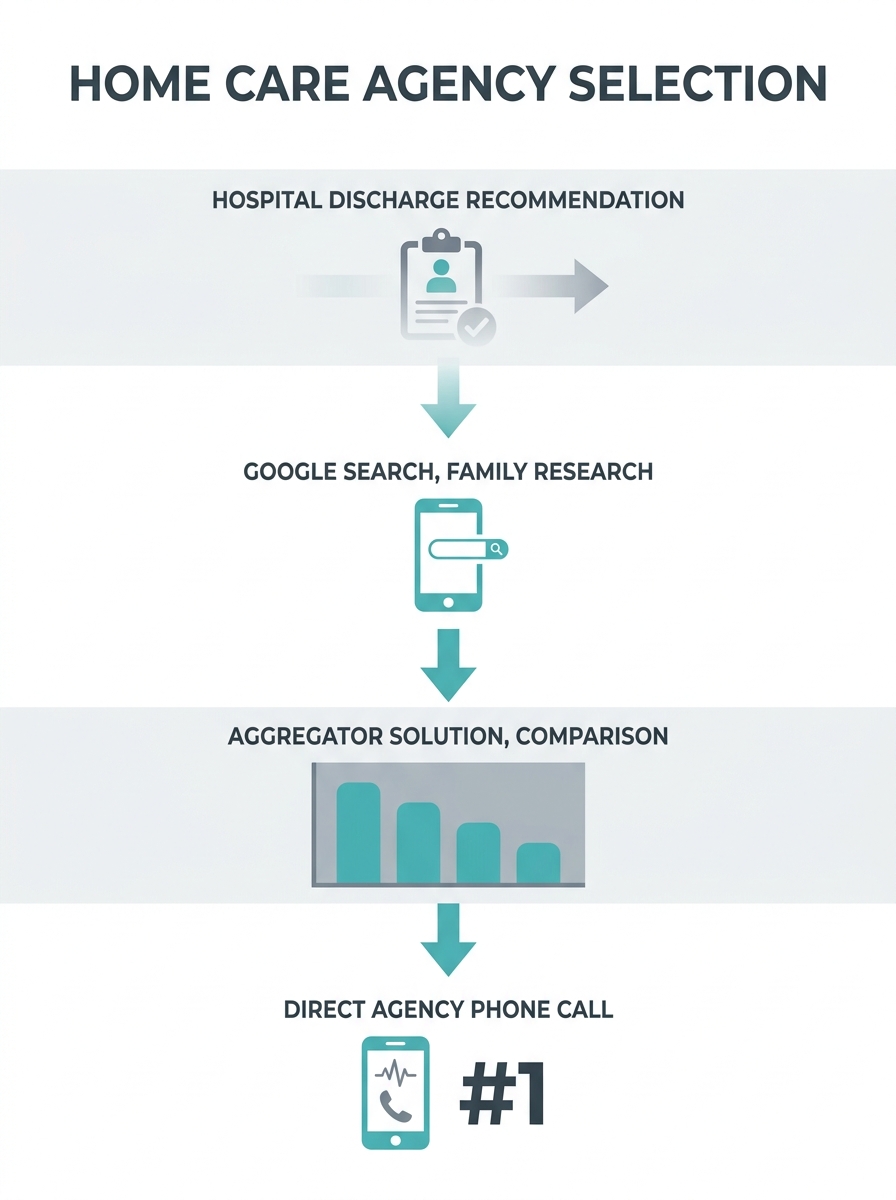
A hospital discharge planner mentions your agency’s name to a patient’s daughter. She goes home, Googles your agency, clicks on your site, reads a few pages, and leaves. Two days later she sees your name again on a list from A Place for Mom. She calls your intake line. Your dashboard records her as an organic Google lead, or maybe as an A Place for Mom referral, depending on what the intake coordinator asks and how the daughter answers. The discharge planner who started the entire chain gets zero credit. Your next budget meeting proceeds with no awareness that hospital relationships generated the lead, and your investment in that referral partnership goes undefended.
This is the core blindness in most agency dashboards. They capture the last touchpoint before conversion and treat it as the whole story. Marketing ROI measurement for home care demands a fuller picture, but the tools most agencies use aren’t configured to provide one. Healthcare marketing dashboards can centralize channel performance into one view, which is a real improvement over checking five separate platforms. But consolidating transactional data from multiple channels still doesn’t solve the attribution problem if each channel is only credited for the conversions it happened to touch last.
How Referral Attribution Breaks in Practice
Referral attribution modeling fails at three specific points in most home care operations, and understanding where each break occurs matters more than selecting the right software. The first break happens at intake. Your intake coordinator is focused on scheduling, collecting insurance information, and making a stressed family member feel heard. Asking “how did you hear about us?” is an afterthought, and the answer is unreliable even when it’s collected. Families often can’t recall the first place they encountered your name, or they cite the most recent touchpoint because it’s top of mind. If this field is a free-text box in your CRM rather than a structured dropdown with defined categories, you’ll end up with dozens of spelling variations of the same source that make any aggregate analysis meaningless.
The second break happens between your marketing tools and your client management system. Your CRM knows who became a client. Your ad platform knows who clicked. Your call tracking software, if you have one, knows who called. But these systems rarely talk to each other in a way that stitches together a single person’s full path. Creating a unified data layer where every ad click, impression, and conversion flows into a central system is the stated goal of modern healthcare marketing tracking, but most home care agencies don’t have the technical infrastructure or staff time to build and maintain those integrations. The result is that your referral pipeline visibility stays fractured across three or four tools, each holding a piece of the picture.
The discharge planner who started the entire chain gets zero credit, and your investment in that referral partnership goes undefended at the next budget meeting.
The third break is conceptual. Traditional digital marketing metrics assume a linear path: impression, click, form fill, conversion. Referral-driven acquisition doesn’t follow that path. A referral from a geriatrician or a hospital social worker might not touch your website at all. The family calls directly because they trust the person who recommended you. These offline referral conversions are invisible to any dashboard that depends on UTM parameters and cookie tracking, which means your highest-trust, highest-converting channel often shows the weakest numbers on your reports. Agencies that base budget decisions on these incomplete reports end up defunding the very relationships that produce their best clients.
Assembling an Attribution Layer That Reflects the Real Pipeline
Building real client source analytics requires changes in process, not just technology. The first and most impactful change is restructuring your intake form. Replace the free-text “how did you hear about us?” field with a two-part question: a required dropdown listing your known referral sources by category (hospital partner, physician office, online search, paid ad, family or friend recommendation, senior living community, aggregator site) and a follow-up field for the specific name or location. This seems minor, but it’s the difference between data you can aggregate and data you can’t. Every coordinator on your team needs to understand why this field matters, because if they skip it during a busy intake call, the entire downstream analysis breaks.
The second change involves connecting your phone system to your marketing data. Platforms like Liine and CallRail assign unique tracking numbers to different marketing channels and referral sources, so when a family calls, you know which campaign, webpage, or even which web design landing page drove the call before the coordinator picks up. Call tracking won’t solve the offline referral problem entirely, but it closes the gap between your digital marketing spend and actual phone conversions, which is where most home care agencies lose the thread. Agencies already dealing with paper-based overhead eating coordinator hours should consider call tracking as part of the same operational cleanup.
The third change is the one that most dashboards never attempt: tracking referral source performance over time, not just at intake. When you know that clients referred by a specific hospital discharge planner convert at twice the rate of clients who find you through paid search, and that those referred clients stay on service an average of four months longer, you can calculate a referral source lifetime value that dwarfs any per-click metric. Referral tracking dashboards built for healthcare providers can monitor incoming pipeline, processing status, and conversion rates across sources, giving you the kind of granularity that makes referral partnership investment defensible in budget conversations. Combining that pipeline data with your retention numbers from your CRM turns referral attribution from a backward-looking report into a forward-looking planning tool. This is where email marketing for care providers can play a supporting role, too: automated nurture sequences segmented by referral source let you track which segments respond to follow-up communication and which go quiet, adding another layer of signal to your attribution data.
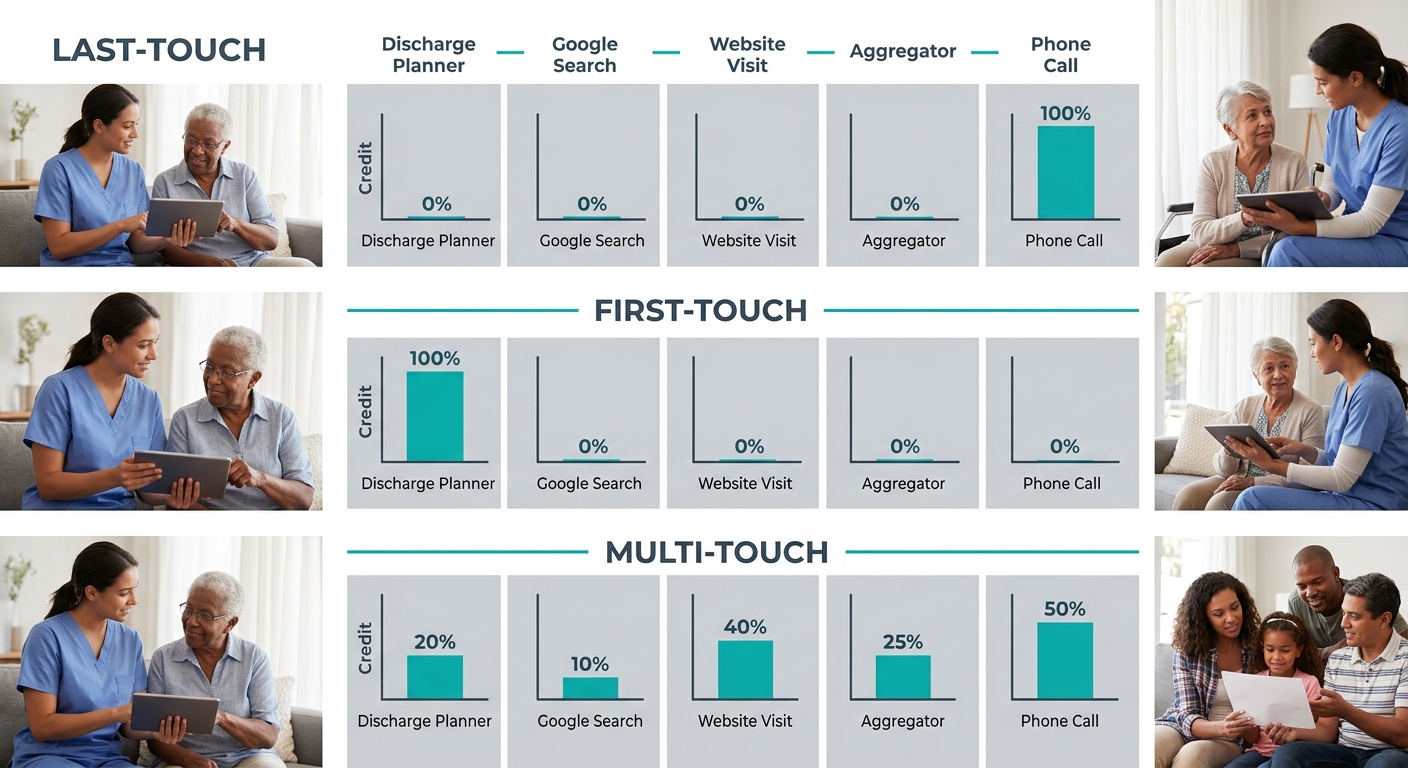
You don’t need to adopt a data-driven algorithmic model on day one. A position-based approach that gives meaningful credit to both the first touchpoint and the converting touchpoint, with smaller credit distributed across middle interactions, is a realistic starting point for most agencies. The key is moving beyond last-touch attribution, which systematically undervalues your referral partnerships and overvalues whatever channel happens to be the final click before a call. Once you can see that pattern clearly in your own data, you’ll understand why your previous dashboard felt like it was telling you a story with the most important chapters ripped out.

Agencies that understand how families choose care providers based on trust signals already know that the emotional weight of a personal recommendation outperforms any ad creative. The attribution system’s job is to make that knowledge visible in the same reports where your paid media performance lives, so your team stops treating referrals as a soft, unmeasurable category and starts treating them as a channel with trackable ROI.
Where This Framework Still Falls Short
Even a well-built client-source attribution system carries blind spots that are worth naming honestly. Multi-touch models assign credit across touchpoints, but they still depend on those touchpoints being observable. When a family member hears your agency’s name at a church group, mentions it to her sister, and the sister calls you three weeks later, there’s no tracking pixel that captures that chain. The offline, word-of-mouth referral path will always have an irreducible fog around it, and any attribution model that claims otherwise is overpromising.
There’s also a tension between attribution precision and the privacy expectations of the families you serve. Healthcare marketing operates under HIPAA constraints that limit how aggressively you can track individuals across platforms. Tools like Freshpaint exist specifically to bridge ad performance and real outcomes in a privacy-compliant way, but the regulatory landscape keeps shifting, and agencies need to stay cautious about how much behavioral data they’re stitching together. The families walking through your door are often in crisis. They deserve to feel like your organization is focused on helping them, not surveilling their browsing history.
And then there’s the resource question. Building and maintaining an attribution layer takes time from people whose schedules are already full. A home care agency with fifteen caregivers and one office coordinator can’t dedicate analyst hours to maintaining UTM taxonomies and CRM integrations. For smaller agencies, the realistic version of this framework might be a well-structured intake dropdown, a basic call tracking setup, and a quarterly manual review of which referral sources produce clients who stay longest. That’s less elegant than a unified dashboard with real-time multi-touch modeling, but it’s infinitely better than the blank “how did you hear about us?” field that most agencies are working with today. The goal isn’t a perfect model. The goal is one that’s honest enough to show you where your clients actually come from, so you can invest your limited marketing budget in the relationships and channels that earn the most trust.


