Caring.com, SeniorAdvisor.com, and A Place for Mom’s Family Lead Program generate pay-per-lead referrals that appear in your CRM automatically. The community figures who shape family decisions months before anyone searches online (estate attorneys, parish nurses, fiduciary accountants) almost never do. Influence center mapping finds and activates those hidden sources.
TL;DR: An influence center is any person or organization families trust during care decisions who falls outside traditional referral channels. Mapping these secondary referral partners, scoring them on reach, trust density, and reciprocity, and building structured outreach cadences turns invisible community stakeholder engagement into your most defensible source of home care lead generation.
Referral customers carry a 16% higher lifetime value and a 13.2% higher spending rate than non-referral customers, according to aggregated B2B referral data. And 84% of B2B decision makers start their buying process with a referral from someone they know. Those numbers apply with even more force in senior care, where the emotional stakes make trusted recommendations the dominant conversion driver. The 6 rules below give you a repeatable system for referral source discovery that competitors relying on paid platforms alone will struggle to match.
Define influence centers by the family’s decision path, not your service category
Capital Group’s practice management research puts it plainly: “What a COI is differs depending on whom you ask. So start by defining your terms.” That advice matters because most agencies define referral partners by healthcare role (discharge planner, physician, social worker) and stop there.
Influence center mapping works differently. You trace the family’s actual decision path backward from intake. When a daughter in Phoenix decides her mother in Tucson needs home care, who did she talk to first? Often it’s a financial advisor reviewing Mom’s retirement accounts, an elder law attorney drafting a power of attorney, a church deacon who visited the home, or a pharmacist who noticed prescription confusion during pickup. ChamberForge’s referral strategy guide confirms that “centers of influence are not solely occupation based” and recommends using your target demographic as a guide instead.
For agencies offering marketing for palliative care or hospice services, the influence map shifts further: grief counselors, oncology nurse navigators, and funeral home pre-planning directors all become primary influence centers. The rule holds regardless of service line. Define the center by where the family actually turns, not where your industry training says to look.

Audit your intake records before building a single new relationship
The temptation is to start networking immediately. Resist it. Your existing intake data already contains the influence map you need. Rough Notes’ referral strategy framework advises practitioners to “consider individuals who have referred you in the past, whether they are clients, COIs, family, friends, or underwriters. List their names and identify any commonalities among them.”
Pull 12 months of intake records. For every client who converted, answer 3 questions: How did they hear about you? Who else was involved in the decision? Did anyone specific recommend the call? You’re looking for the “invisible hand” referrals, the names that surface 3 or 4 times across unrelated families. One agency owner discovered that a single financial planner at a regional Edward Jones office had influenced 7 of her 45 new clients in a year, and she’d never once contacted that planner directly.
GetTheReferral’s research reinforces this approach: “Get input and referral ideas from the different departments inside your company.” Your schedulers, care coordinators, and field caregivers hear things during home visits that your marketing team never captures. Survey at least 4 internal departments (intake, scheduling, field supervision, billing) with a simple prompt: “Which non-medical professionals do families mention by name?” The patterns will surprise you.
If you’ve already built a referral partner portal or CRM infrastructure, check whether your secondary referral partners even appear in those systems. They usually don’t.
Score every potential influence center on reach, trust density, and reciprocity
Why does a scoring framework matter here? Because an estate attorney who handles 200 elder law cases per year and a yoga instructor who teaches 1 chair yoga class per week are both “influence centers,” but they require completely different investment levels. You need a way to prioritize.
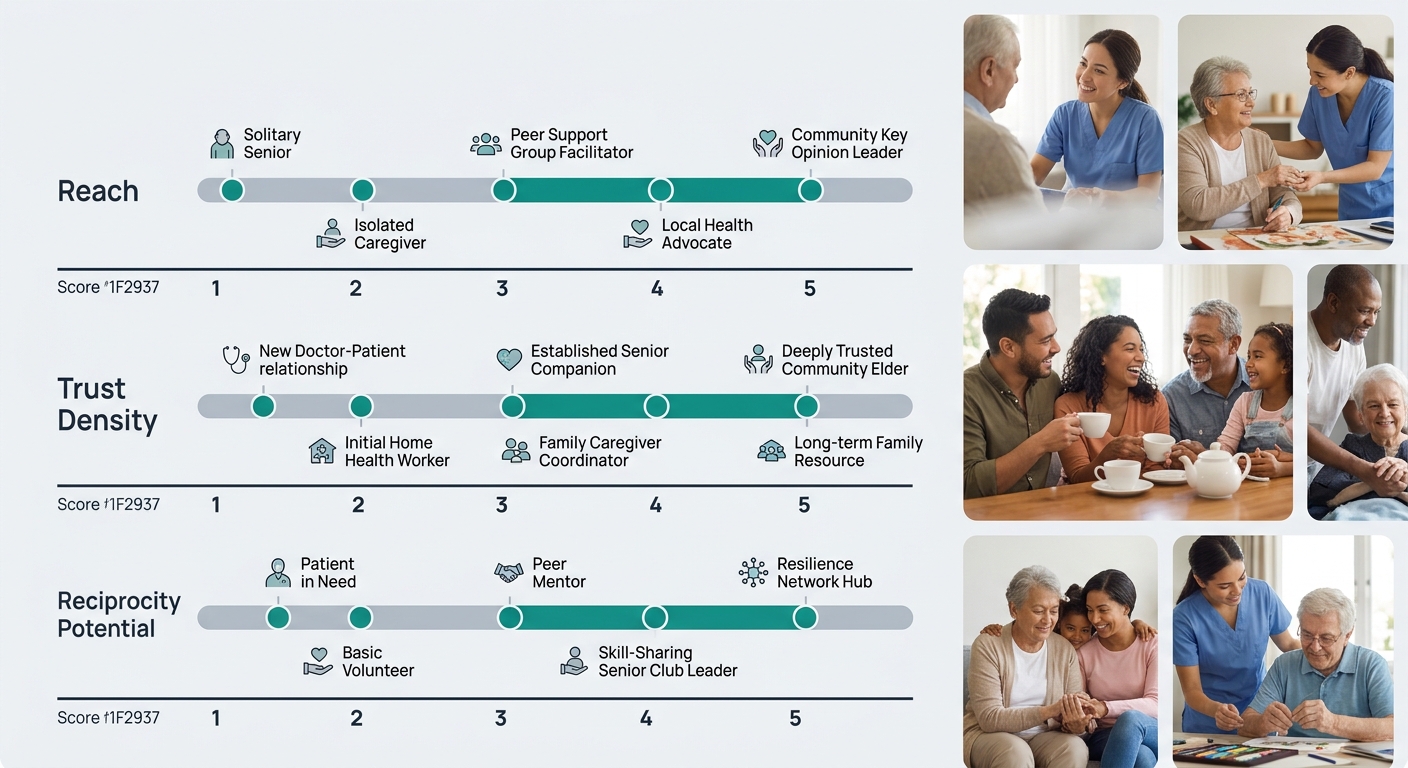
The Influence Center Scoring Model evaluates each potential center on 3 axes:
| Scoring Axis | What It Measures | High Score Example | Low Score Example |
|---|---|---|---|
| Reach | Volume of families the center interacts with annually | Financial planner managing 150+ retirement accounts | Neighbor who helped 1 family |
| Trust Density | Depth of trust families place in this person’s recommendations (92% of people trust referrals from those they know) | Elder law attorney advising on POA and asset protection | Generic online review site |
| Reciprocity Potential | Can your agency send value or referrals back to this center? | Home health aide flags legal needs back to the attorney | One-directional paid lead platform |
Score each axis from 1 to 5. Any influence center scoring 12 or above (out of 15) deserves dedicated outreach. Centers scoring 8 to 11 get quarterly touchpoints. Below 8, monitor passively. This prevents the common mistake of spending equal energy on every contact, which dilutes your effort across dozens of low-yield relationships.
Tip: Run this scoring exercise for your top 20 influence center candidates. Most agencies find that only 5 to 8 score above the 12-point threshold where dedicated outreach makes financial sense.
Lead with clinical value before mentioning referrals
Commonwealth’s advisor guide on building center-of-influence relationships states: “Establish your credentials and show how dedicated you’d be to serving their clients’ best interests. Make it clear that you are committed to being a mutual source of referrals.” The order of those two sentences matters. Credentials and dedication come first. The mutual referral commitment comes second.
Too many agency owners walk into an elder law office, hand over a business card, and ask for referrals within 10 minutes. That approach has a near-zero conversion rate. Instead, lead with something the influence center’s clients actually need. Offer a free fall-risk assessment checklist their staff can hand to clients. Provide a 1-page guide on what Medicare Part A and Part B cover for home health (a question every estate attorney’s clients ask and the attorney can’t answer). Create a medication management reference sheet for the pharmacist’s counter.
These aren’t marketing brochures. They’re clinical tools that make the influence center look more knowledgeable to their own clients. That value exchange builds the reciprocity your scoring model measures. Agencies working on marketing for caregiving agencies will find that educational content about caregiver qualifications, background check processes, and supervision protocols gives influence centers concrete talking points when families ask “How do I know this agency is safe?”
We’ve written before about why your strongest client advocates aren’t always your best growth channel. The same logic applies here. The best influence centers aren’t the ones who love you most. They’re the ones positioned to intercept families at the moment of decision.
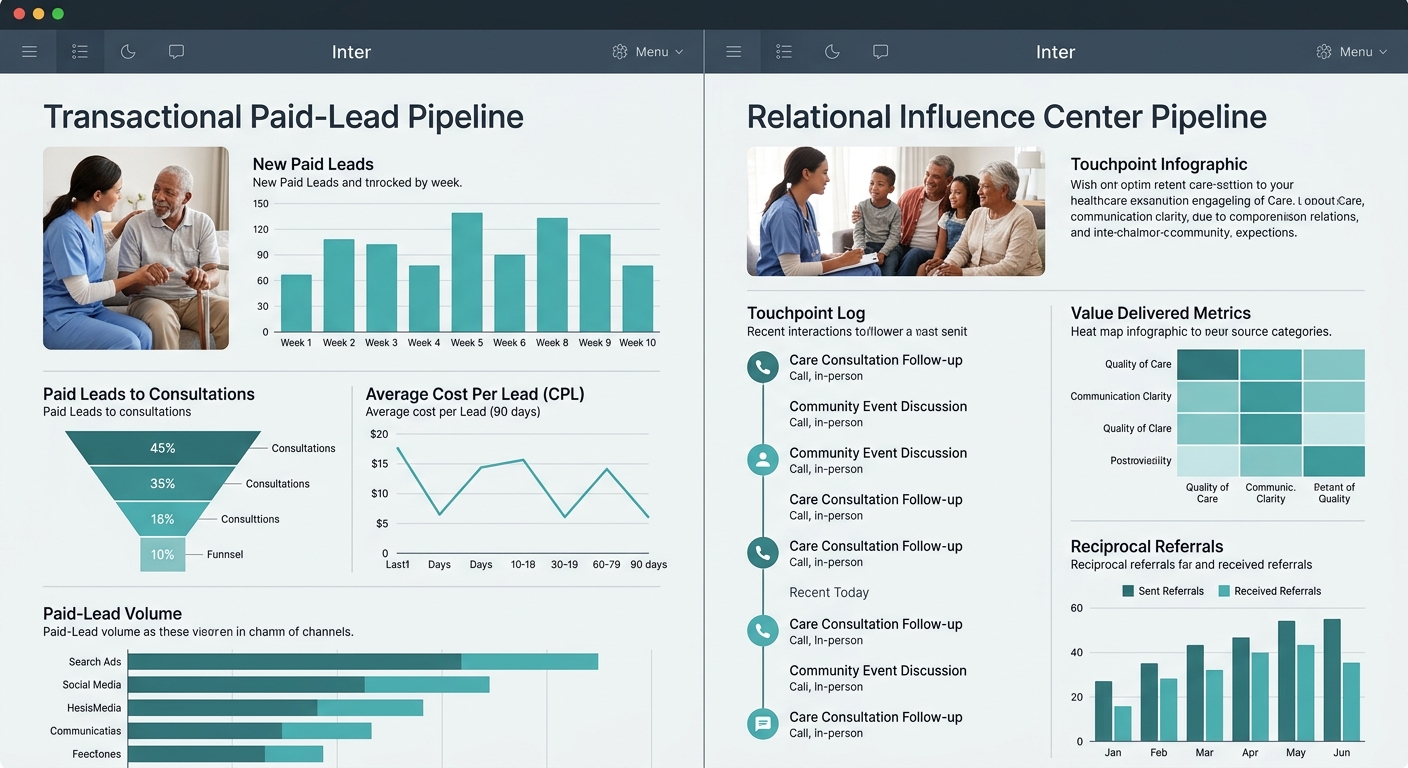
Track influence centers in a separate pipeline from paid lead sources
Paid platforms like A Place for Mom operate on a pay-per-lead model with what they describe as 100% verified leads, no long-term contracts, and no monthly fees. That’s a transactional pipeline. Influence center relationships are relational pipelines. Mixing them in the same CRM view creates 2 problems: you measure them against the same cost-per-acquisition benchmarks (which penalizes slow-building relationships), and you lose visibility into which community touchpoints are producing compounding returns over 6, 12, and 24 months.
Create a dedicated CRM tag or pipeline stage for influence centers. Track 4 metrics per center: number of introductory touchpoints completed, pieces of clinical value delivered, referrals received (with source attribution), and referrals sent back to the center. That last metric matters more than most agencies realize. A financial planner who receives 3 warm introductions from your agency in a quarter is 4 to 5 times more likely to reciprocate than one who only receives thank-you emails.
The best influence centers aren’t the ones who love you most. They’re the ones positioned to intercept families at the moment of decision.
If your team is also investigating why existing referral relationships stall after the first meeting, separate tracking reveals whether the issue is follow-up cadence, value delivery, or misaligned scoring from the start.
Make your networking cadence contractual, not aspirational
“I should reach out to that attorney” is an intention. “Every second Tuesday, our liaison contacts the top 5 influence centers with a relevant clinical update” is a system. The difference between agencies that build durable influence networks and those that don’t comes down to cadence discipline.
For high-scoring centers (12+ on the model), schedule contact every 2 weeks. That doesn’t mean a sales pitch every 14 days. Rotate through 4 contact types: a brief email with a useful clinical resource, an in-person drop-in with printed materials for their waiting room, a phone call to ask what questions their clients have been raising, and a quarterly co-hosted educational event (even a 30-minute lunch-and-learn counts). For mid-tier centers (scores of 8 to 11), shift to monthly contact with the same rotation.
Block 4 to 6 hours per week on your marketing liaison’s calendar specifically for influence center outreach. If that time isn’t protected, it gets consumed by intake calls and administrative work within days. Agencies offering assisted living marketing alongside home care services can double the value of each contact by positioning themselves as a resource for the full continuum of care, which gives influence centers a single point of referral for families with varying needs.
When These Rules Break Down
These rules assume your agency operates in a geography with enough professional density to map meaningful influence centers. In rural markets with fewer than 3 elder law attorneys and 1 or 2 financial planning offices within 30 miles, the scoring model compresses. Everyone scores lower on reach, and you end up working with centers that would fall below threshold in a metro area.
The fix in rural settings is expanding the definition of “center” further into civic life: postmasters, volunteer fire department leadership, county extension agents, and Feed & Seed store owners who know every family on their route. The scoring axes still apply, but the thresholds drop. A center scoring 9 in a rural county with 12,000 residents may carry more actual influence than one scoring 13 in a metro county with 900,000.
The other breakdown point is compliance. If your agency participates in Medicare-certified home health, the Anti-Kickback Statute constrains what you can offer influence centers in exchange for referrals. Clinical value (educational materials, free assessments for their clients) is generally safe. Gift cards, paid dinners, and percentage-based referral fees are not. Review your influence center outreach plan with counsel before launch, especially given the heightened compliance scrutiny across the industry right now.
These 6 rules give you a structured process for influence center mapping that compounds over time. Paid lead platforms reset to zero every month. An elder law attorney who trusts your clinical team and sends you 2 families per quarter will keep doing so for years, at zero marginal acquisition cost, as long as you maintain the cadence and keep delivering value back.


